Background: Implantable loop recorders (ILRs) were traditionally inserted in the cardiac catheter lab on a consultant-led list. The most modern generation of devices (e.g. Medtronic LINQ II) are designed to be injected subcutaneously. The relative simplicity of the procedure brings it within the skillset of Allied Health Professionals (AHPs), freeing up medical staff, available cath lab time and increases revenue. Nottingham University Hospitals NHS Trust (NUH) setup the AHP ILR service in September 2017 with two AHPs, and currently operates with four as the demand for the elective service has grown, having more than quadrupled in 5 years.
Method: The setup of the AHP service involved training one cath lab practitioner and one cardiac physiologist under consultant supervision. After initial training, the lists were performed independently with a consultant available if necessary. As the demand for the ILR service has grown, the team has had a total of 9 AHP staff trained as implanters throughout the 5 years, and currently consists of two cath lab nurses and two cardiac physiologists. Each elective list typically runs with two trained members of staff. Patients no longer receive a preadmission, nor are antiplatelets/anticoagulation routinely stopped. The patients are ambulatory, not fasted and do not receive antibiotics for the procedure. Most patients are discharged within one hour of their scheduled appointment time.
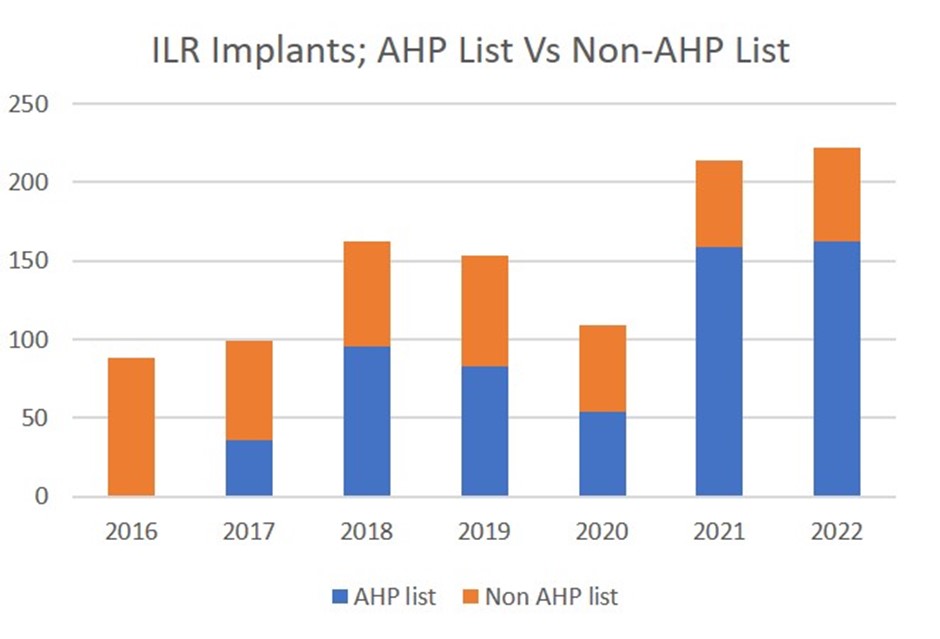
Results: Since 2016, NUH have implanted 1,008 ILR devices, with 62% of these on elective AHP lists. In that time, we have recorded 9 device infections – 0.89% complication rate (0.47% AHP list versus 1.5% non-AHP list; Fisher’s exact P=0.59) and 6 device erosions – 0.59% complication rate (0.79% AHP list versus 0.26% non-AHP list Fisher’s exact P=0.42). Elective AHP lists currently account for 75% of ILRs implanted in NUH. The AHP staff currently perform 70% of inpatient ILR procedures. 23% of people who had an ILR went on to have a further procedure, such as a pacemaker or catheter ablation based on findings from the ILR. The skill of the implanters means that 3 of the AHP staff have been trained autonomously by existing AHP implanters without the need for consultant input.
Implications: The AHP loop recorder implant service is safe and cost effective. Implant volume is increasing. We are now able to train further AHP implanters independent of consultant supervision to meet the increased demand on the service. ❑
Figure 1: ILR implants: AHP list versus non-AHP list