Introduction: Implantable cardioverter defibrillators (ICDs) reduce mortality in people at risk of sudden cardiac death. During ventricular tachycardias (VT), cardiac output is reduced due to fast heart rates reducing diastolic filling time, loss of atrio-ventricular synchrony and loss of bi-ventricular synchrony.
Improving haemodynamic status during VT may allow more time for VT to self-terminate and postpone the need for acutely lifesaving, yet paradoxically harmful therapies in the longer term.
Patients requiring ICDs often have a pacing indication. In those at high risk of developing pacing-induced cardiomyopathy, conduction system pacing is often now preferred over right ventricular pacing, and additionally is rapidly gaining traction for its use as a heart failure treatment.
We assessed the potential benefit of His bundle pacing as a therapeutic approach to improve cardiac output during ventricular tachycardia (VT) and also its ability to terminate VT.
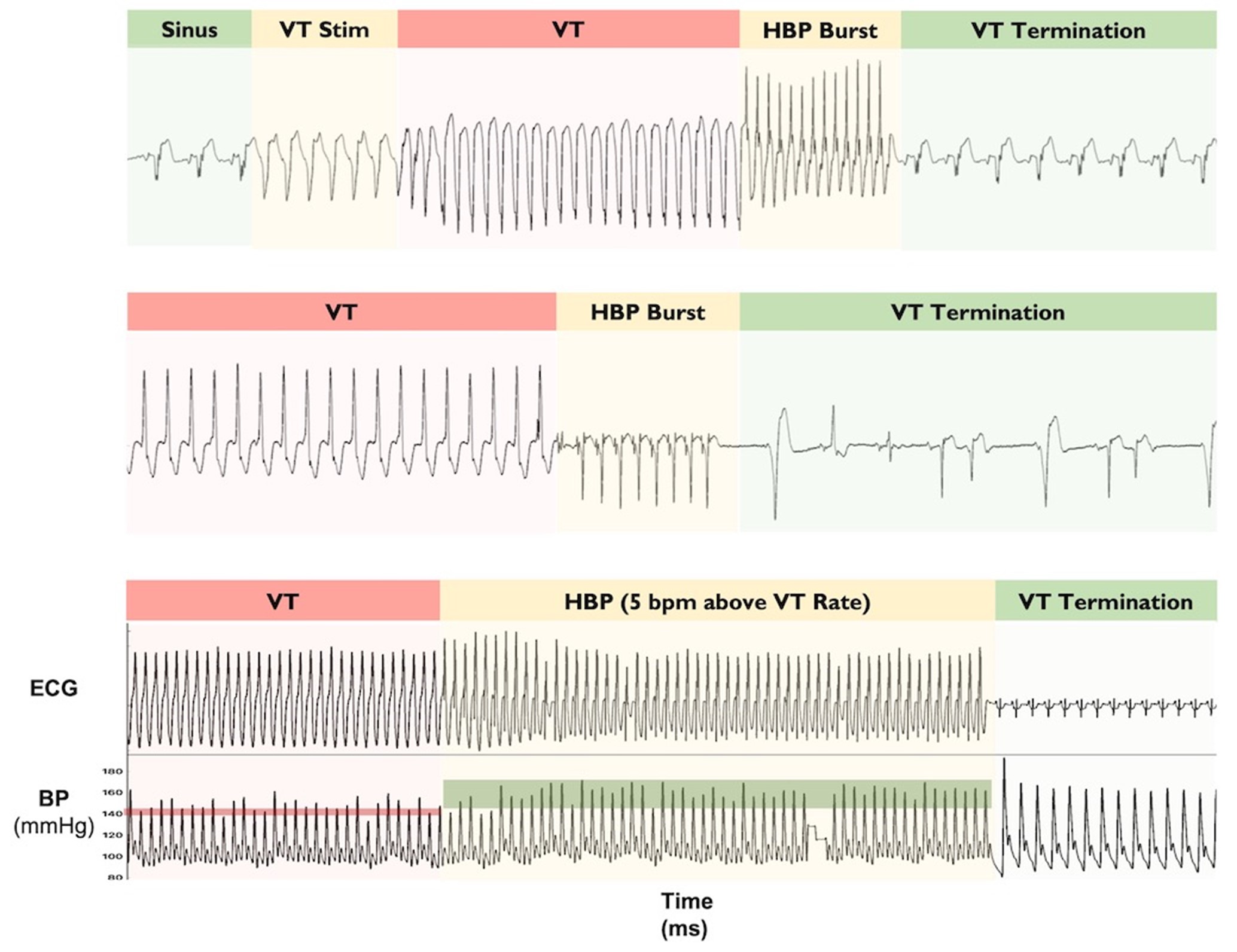
Methods: Patients attending for clinically indicated invasive electrophysiology procedures who experienced clinical VT (either spontaneously or induced with a ventricular drive train and shorter coupled S2 and S3 beats) were recruited. We recorded a continuous 3-lead ECG and beat-by-beat blood pressure (either invasively or non-invasively with a Finometer). After around 15 seconds of clinical VT, we paced the His bundle at 5 bpm above the VT rate to assess the haemodynamic response. We measured the percentage change in systolic blood pressure during His bundle pacing relative to the systolic blood pressure during clinical VT.
After achieving termination in 2, the protocol was adapted for the final 4 patients to deliver a short burst of His bundle pacing (8–15 beats) at 91% of the tachycardia cycle length.
Results: Ten patients with clinical VT were recruited. Ninety per cent were male with a mean age 71, and mean LVEF 28%. Half had ischaemic cardiomyopathy, and the mean clinical VT rate was 142 ± 21 bpm.
His bundle pacing during clinical VT increased systolic blood pressure by +14.2% (CI: 7.8–20.6; p=0.0023). Once entrained, the interval from stimulus to QRS onset was 45 ± 18 ms, in keeping with ventricular activation via the His-Purkinje system.
In 6 of 10 patients, VT terminated with His bundle pacing without accelerating VT or developing VF.
Conclusions: His bundle pacing during clinical VT can improve haemodynamic function and even terminate VT episodes. Further study is required to (1) confirm these findings, (2) to optimize the therapeutic pacing approach and (3) to compare efficacy against ATP delivered from the RV. ❑
Figure 1