Introduction: Over the past 10 years, the indications for implantable loop recorder (ILR) have broadened and the device size has reduced substantially. The implant procedure has moved from the physician-led catheter-lab environment to non-physician-led outpatient procedures. ILR explant procedures have not transitioned in parallel. We implemented a non-physician, outpatient ILR explant service in 2021 and hypothesized that the new explant method of a non-physician explant service performed in outpatients would have comparable safety outcomes and procedural times.
Methods: Patients over the age of 18 undergoing and ILR explanation during the period of July 2016 to January 2023 were included. Data was collected prospectively at the time of explant and during patient follow up 1 week post procedure. Written consent for the procedure was obtained for all patients. The study was registered and approved by the Clinical Effectiveness Unit at Barts Heart Centre (ID: 13317). Procedures were performed in an outpatient clinic room with a member of clinical support team or nursing assistant assisting the procedure. Wound closure was at discretion of the explanator with an option of wound closure strips or dissolvable sutures. No patients were asked to withhold medications prior to procedure, and post procedure, patients were asked to wait 20 minutes in the shared waiting area to ensure no bleeding complications occurred. Like ILR implant procedure, sterile gloves are worn without the requirement of a surgical gown to reduce stress for the patient.
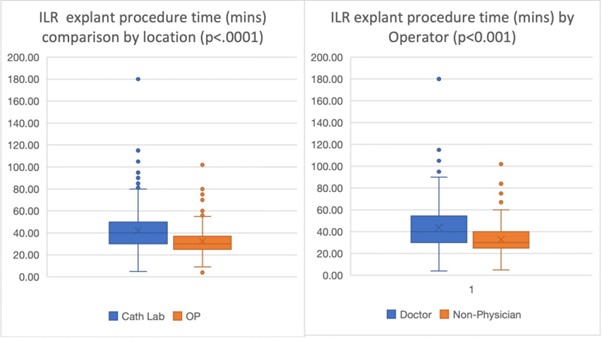
Results: Seven hundred and forty-two patients were included during the study period with 594 (80%) being performed in the catheterization lab and 504 (68%) being performed by doctors. Four (0.5%) late complications were noted; all these patients’ procedures were performed in the catheterization lab by doctors. These late complications were 2 wound infections and 2 stitch protrusions that required re-intervention. ILR procedures performed in the catheterization lab were significantly longer procedures, and significantly shorter when performed by non-physicians.
Conclusions/implications: This study has shown that ILR explants can be performed safely in an outpatient setting by non-physicians, with an improvement in procedural time. This study did not include time in the hospital, which would have been significantly longer due to admission and ‘recovery’ post-procedure. The outpatient model only utilises a 20-minute waiting time, that is self-directed by the patient in a shared waiting area post procedure. Reasoning for the procedure time being significantly shorter could be due to the number of operators that were performing the procedures in each group. Over 100 operators performed procedures in the doctor group with only 5 non-physicians. This ‘sub-specialization’ of a lower volume of operators for specific procedure could provide consistency and improve efficiencies. ILR explant procedures being performed by non-physicians enables them to carry out more complex procedures, such as pacemakers. ❑
Figure 1