Introduction: In patients eligible for cardiac implantable electronic device (CIED) placement with the need of a high percentage of ventricular pacing, early indication for CIED placement able to deliver cardiac resynchronization therapy (CRT) is advantageous, because it may prevent a pacemaker syndrome (left ventricular ejection fraction deterioration in patients with apicoseptal right ventricular lead placement and high percentage of ventricular pacing).Bundle branch area pacing are evolving techniques taking the approach of physiological excitation using the heart’s intrinsic conduction system. This potentially enables complete cardiac resynchronization without the need for left ventricular lead placement. In current literature, the outcome of physiologic pacing is comparable to pacemakers able to deliver cardiac resynchronization therapy. Compared to upper His bundle pacing, stimulation of the left bundle has a better response, more stable pacing thresholds and better success in correcting pre-existing bundle branch blocks. This is a reason why His lead placement is occasionally supported by mapping of the area of interest. This, however, expands both the procedure time and its complexity. In our case series, we highlight a new approach.
Methods: Every consecutive patient eligible for CRT placement, where coronary sinus (CS) lead placement was not possible underwent right ventricular target area mapping. In order to map the area of interest, the respective lead (which could be a CS lead or a His bundle lead) was implemented into our mapping system ESI NavX (Abbott) by connecting it to the system with an alligator clip (Figure 1) and used as the mapping catheter.
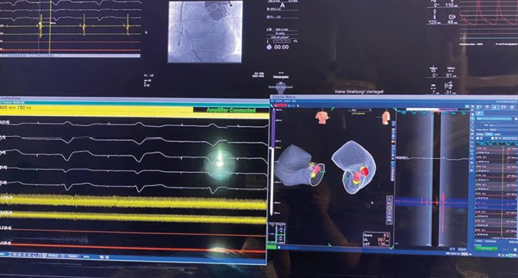
The helix was deployed partially and its tip was used to high-density map the target area. An intracardiac ECG was used to record the cycle length after excitation to identify the optimal position for placement of the lead tip (Figure 2).
The helix was then fully deployed and the respective lead placed. Primary endpoint was change of pacing threshold and RV–LV delay during 12-months follow-up. Secondary endpoints were adverse events of all grades and all-cause mortality.
Results: Between March 2022 and January 2023, a total of 8 participants (6 male) aged 79.25 years (73–90) underwent our specific map/pace procedure. Mean procedure time was 80.75 minutes (49–115). Mean follow-up time was 273.5 days (35–458). During follow-up pacing, thresholds were stable in all participants. Altogether, 6 adverse events were observed, unrelated to the procedure or the CIED. One participant succumbed during bypass surgery.
Discussion/conclusions: Physiologic pacing has evolved as an alternative to conventional pacing methods with placement of an RV lead in the anteroseptal position. Specific leads are able to deliver cardiac resynchronization, even without placement of a CS lead. Placing the lead optimally may be burdensome in terms of finding the ‘sweet spot’. Enhancing the response rate via mapping of the left ventricle in case of CS-lead placement or the right ventricle in case of His-lead placement has been reported. Our procedure combines the advantages of being able to map the area of interest for a perfect response rate, and at the same time lowers the procedure time and the cost due to implementation of the lead into the mapping system, when compared with conventional mapping techniques. Our procedure is effective, safe and cost effective. ❑
Figure 1: Alligator clips

Figure 2: Intracardiac ECG and map during lead placement