Background: Conventional radiofrequency (RF) ablation for atrial fibrillation (AF) can cause significant patient discomfort even under mild conscious sedation (mCS), contributing to the predominant use of cryoablation (Cryo) for pulmonary vein isolation (PVI). We hypothesized that by reducing energy delivery times, a very high-power short-duration (vHPSD) RF protocol could offer a patient experience comparable to Cryo.
Method: Two UK tertiary cardiac centres prospectively recruited consecutive patients undergoing first-time AF ablation under mCS using intravenous paracetamol, fentanyl or morphine, and midazolam, using either vHPSD (90W lesions delivered for up to 4 seconds) or Cryo. For vHPSD, left and right wide antral circumferential ablation was performed with contact force sensing using Q Mode Plus and the QDot Micro catheter (Biosense Webster). In the Cryo group, Arctic Front Advance Pro (Medtronic) or Polar X (Boston Scientific) catheters were used to deliver lesions for up to 4 minutes at a time. PVI was confirmed at procedure end. All patients were asked to complete standardized questionnaires between 4–24 hours post-ablation, using Likert and visual analogue scales (VAS) to assess the anxiety, discomfort and pain that they had experienced. Operators and nursing staff also completed similar questionnaires immediately after each procedure to record their assessment of the patient’s intraprocedural status.
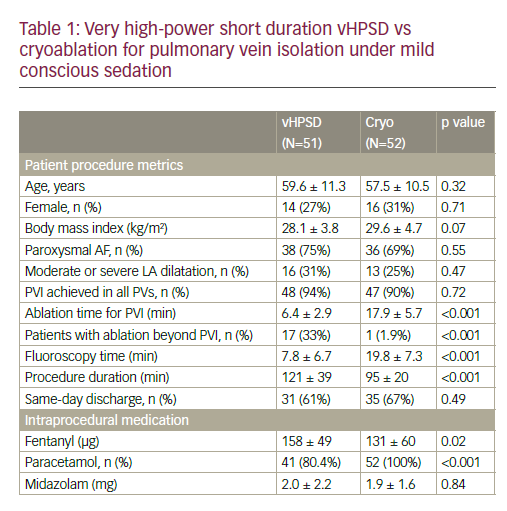
Results: A total of 103 patients were included (51 vHPSD, 52 Cryo). Their procedural metrics and intraprocedural medications are summarized in Table 1. Rates of successful PVI were similar, with vHPSD having lower ablation duration to achieve PVI (6.4 ± 2.9 min vs 17.9 ± 5.7 min; p<0.001) and lower fluoroscopy time (7.8 ± 6.7 min vs 19.8 ± 7.3 min; p<0.001) compared with Cryo. Overall procedure duration was greater for vHPSD (121 ± 39 min vs 95 ± 20 min; p<0.001), which was unchanged after excluding cases with non-PV ablation (110 ± 35 min vs 95 ± 20 min; p=0.024). Patient experience was comparable for vHPSD and Cryo (Figure 1A). Nurse VAS estimations of discomfort and pain were greater than the patients’ own scores (discomfort: p=0.02 for vHPSD, p=0.03 for Cryo; pain: p=0.007 for vHPSD, p=0.013 for Cryo). Patient willingness to have the same experience for a repeat ablation did not differ between groups (Figure 1B).
Conclusion: The patient experience of vHPSD RF ablation for AF under mCS was comparable to Cryo. vHPSD ablation was associated with reduced overall ablation times and reduced fluoroscopy exposure, and similar rates of same-day discharge. Nurses make a crucial contribution to patients’ experience through greater sensitivity to their intraprocedural needs. ❑