

Introduction: We introduced RETRO-mapping as a software for mapping activation during atrial fibrillation (AF). We subsequently suggested features, such as cycle length (CL) and conduction velocity, to detect plane activity. In this work, we suggest an algorithm for automatic classification of wavefronts. We also explore the relationship between CL and degree of organization of activity.
Methods: We recorded electrograms from 9 patients in AF using a 20-pole spiral catheter to create the 2D representation of RETRO-mapping. We defined four types of wavefronts (plane, focal, collision, and rotational), based on the number of endpoints and number of edges. A plane wavefront has a single edge with two endpoints at the limit of the field of view throughout the wavefront, as in Figure 1. For a collision wavefront, the number of edges and the number of endpoints both decrease over time. Focal wavefronts, which have a role in initiating paroxysmal AF,1 have a single edge but no endpoints, e.g. a circle. A rotational wavefront has a single edge with 2 endpoints, where 1 endpoint is in the centre and the other at the limit of the field of view. Classification results of 48,567 activation edges were validated against a clinician’s judgement.
Results: Table 1 gives the percentage of each type of wavefront per case. Patients with persistent AF treated with amiodarone had on average the lowest percentage plane activity. A linear regression between median CL and percentage plane activity returned an R2 value of 0.72. The interquartile range of CL was significantly higher for patients with persistent AF treated with amiodarone (the same patients with lower plane activity).
Conclusions: We can use the number of edges and endpoints to classify the type of wavefront using RETRO-mapping. A higher interquartile range of CL correlates to less plane activity, thus may be a measure of disorganization in AF and the effect of amiodarone could be evaluated against current literature findings.2 As this was an initial study of 9 patients, a larger study is needed to validate our initial results. ❑
Figure 1: A sample field of view of RETRO-mapping showing a plane activation edge

Endpoints are shown in green, and the edge is shown in dark red.
Table 1: The percentages of wavefront type
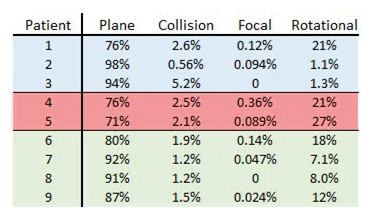
Three patients had paroxysmal AF (blue), 2 had persistent AF treated with amiodarone (red), 4 patients had persistent AF without amiodarone treatment (green).












