

Balloon aortic valvuloplasty (BAV) has experienced a complex evolution in clinical practice, transitioning from an early therapeutic innovation to limited use, and more recently to a redefined role in the era of transcatheter aortic valve implantation (TAVI). While TAVI has transformed the management of aortic stenosis, BAV continues to hold important value in selected clinical scenarios, particularly in high-risk, complex, or resource-limited settings.
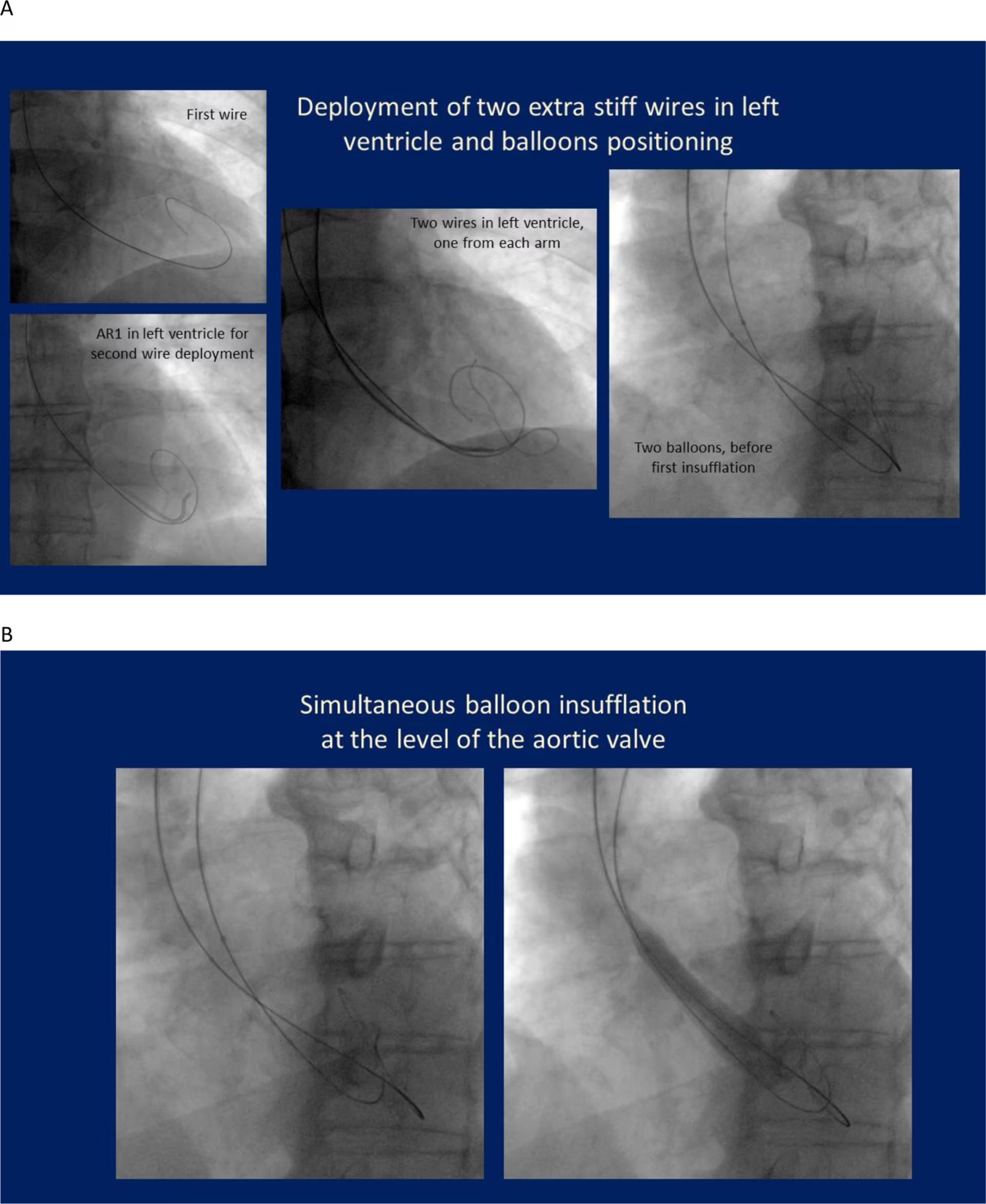
In the first of our new practice pearls series, In Rhythm, Dr Gustavo Samaja (Sanatorio Colegiales, Buenos Aires, Argentina) shares practical insights into the contemporary role of BAV, including patient selection, procedural strategies, and its use as both a bridge and a decision-making tool. He also discusses how evolving healthcare systems and resource considerations continue to shape the balance between BAV and TAVI in everyday clinical practice. Balloon aortic valvuloplasty (BAV) was developed around 40 years ago by Professor Cribier and led to immediate improvement in patients by relieving the transvalvular gradient. However, a few years later, due to vascular complications and a high rate of restenosis, the procedure was largely abandoned and reserved mainly for palliative treatment. With the development of TAVI, valvuloplasty experienced a revival, as it became an important step within a definitive treatment strategy and contributed to an overall increase in its use worldwide. Interestingly, while TAVI initially revitalized valvuloplasty, it is now, in some respects, contributing to its decline, as more clinicians use TAVI directly to achieve the benefits that balloon aortic valvuloplasty once provided across a broad range of clinical situations. We can identify three main groups of patients who may benefit. The first are patients in shock, who require valvuloplasty as part of a definitive treatment strategy. The second group includes patients for whom valvuloplasty serves, in a sense, as a palliative procedure, helping to improve their clinical status and quality of life. Finally, perhaps the most interesting and variable indication is the use of valvuloplasty as a bridge to decision. In these cases, the outcome of valve opening is uncertain, so valvuloplasty is performed to guide further management based on the observed hemodynamic improvement. I believe that BAV should be indicated over TAVI in patients presenting with shock. In recent years, emergency TAVI has been proposed, but in my view BAV remains superior, mainly for three reasons. First is immediate availability: valvuloplasty can be performed within hours, regardless of the situation and available resources, and it can also be carried out in centres without TAVI facilities. The second point relates to understanding the patient. In an emergency setting such as shock, it is crucial to have a comprehensive view of the patient to avoid potential mistakes. However, this is often not possible; you may be unaware of comorbidities, the patient’s overall context, or associated conditions. Perhaps most importantly, the presence and extent of coronary artery disease may be unclear. It is unlikely that a patient with aortic stenosis in shock has no concomitant coronary disease, and determining the optimal strategy for managing this becomes much more difficult once TAVI has already been performed. Therefore, performing a valvuloplasty first allows time to assess and, if necessary, treat coronary disease before proceeding to TAVI at a later stage. The third point concerns procedural risk. Although emergency TAVI can now be performed in relatively low-risk settings, in the context of shock the risk profile changes. There is a higher likelihood of vascular complications, which can be devastating in these patients. In addition, TAVI carries an approximately 10% risk of requiring a pacemaker, which may be particularly harmful in a patient in shock. When BAV is used as a bridge to TAVI, patients generally fall into two opposite groups, with a broad spectrum in between. On one hand, there is the relatively younger patient, for example, a 70-year-old in shock. In this situation, BAV is performed to stabilize the patient and improve their condition, with the clear expectation that TAVI will follow. This does not necessarily mean performing TAVI the next day or even the next week, but it should be planned within a defined timeframe, typically within 1–3 months, bearing in mind the likelihood of restenosis. On the other hand, there is the much older patient, for example, a 95-year-old, in whom BAV is performed primarily to improve symptoms, with the hope that it may serve as a definitive treatment. In these patients, the strategy is to wait and monitor for the recurrence of symptoms rather than planning TAVI upfront. In summary, when BAV is used simply to stabilize a patient who is expected to develop restenosis, TAVI should be anticipated and planned. However, when treating patients where life expectancy and comorbidities are uncertain, it is often more appropriate to adopt a watchful approach. To maintain the role of BAV, it is essential to achieve a low rate of complications, particularly vascular complications. In this regard, the procedure can be performed via the femoral artery using refined techniques, such as avoiding heparin and using low-profile balloons, with good results. However, the most significant advancement has been the use of transradial access. Transradial access offers a safer approach to BAV, as it almost eliminates vascular complications. That said, an important limitation is the small diameter of the radial artery. To achieve optimal results, non-compliant balloons are required, but these cannot be easily delivered through the radial artery. While compliant, large balloons can be used through a 7 or 8 French sheath via transradial access, the procedural results are often suboptimal. Moreover, the patients who would benefit most from transradial access—typically elderly, frail individuals—are often not suitable candidates for such large sheaths. Over the past 20 years, we have developed a programme of bilateral transradial axis valvuloplasty. The idea is to use two peripheral non-compliant balloons, one through each radial artery, and perform a simultaneous insufflation. If only one radial access is available, a combined radial and femoral approach can be used. In my opinion, this represents the optimal BAV technique, offering a low complication rate, a high procedural success rate, and effective gradient relief. In addition, it does not require cardiac pacing, as inflation of one balloon helps stabilize the other. Although advancing two wires into the ventricle can be technically challenging, the overall procedure is straightforward. (a) Two extra stiff 0.035” wires are deployed into the left ventricle through the aortic valve, one from each arm. (b) Simultaneous insufflation of the balloons at the level of the aortic valve. Rapid ventricular pacing is usually not required with this technique. It is important to recognize that BAV equals restenosis; if the patient lives long enough, restenosis will occur. With this in mind, careful follow-up is essential, and clinicians must be prepared either to repeat BAV when TAVI is not suitable or to proceed to TAVI when appropriate. The realistic goal of BAV is immediate symptomatic improvement, and in this respect, the benefits are clear. However, its main limitation remains the inevitable occurrence of restenosis. I think it is less about identifying specific red flags and more about defining an appropriate strategy. In younger patients, the approach should be clear: if you perform a BAV, you should already be considering progression to TAVI. If the patient is not suitable, close follow-up is essential, particularly monitoring ventricular function and, most importantly, symptoms. These patients are rarely lost to follow-up, as they often have concomitant conditions requiring ongoing care. Even when the initial valvuloplasty result is good, TAVI should remain a key consideration in younger patients. In my view, healthcare resources are closely linked to our ability to deliver appropriate care. While some indications are clear-cut, there is a broad spectrum of patients in whom decision-making is less straightforward. In lower-resource settings, BAV plays a particularly important role in avoiding futile interventions. A typical example is the frail patient, in whom proceeding directly to TAVI may ultimately be of little benefit. Performing BAV and observing the clinical response after relieving the gradient can provide valuable insight, helping to determine whether TAVI would be beneficial or futile. The same principle applies in other uncertain scenarios, such as patients with low ejection fraction, where the relative contribution of valvular disease may be unclear, or in patients with ambiguous symptoms. In these situations, BAV can help to guide decision-making and avoid futile procedures. Already registered? Login below.
Q. Could you describe the history of balloon aortic valvuloplasty (BAV) and transcatheter aortic valve implantation (TAVI)?
Q. In the TAVI era, which patient profiles still mainly benefit from BAV and how do you identify appropriate candidates in daily practice?
Q. Do you think that there is a specific clinical situation in which BAV is almost undeniably preferable to TAVI?
Q. When using BAV as a bridge to definitive TAVI, what clinical or hemodynamic parameters help you decide when and whether to proceed with TAVI afterward?
Q. What procedural techniques or refinements have most improved safety and outcomes with modern BAV?
Q. What realistic goals, expected benefits and limitations should clinicians consider when offering BAV as palliative therapy in patients unsuitable for TAVI?
Q. Given the short-lived hemodynamic benefit of BAV, what complications or red flags should clinicians proactively anticipate in follow-up, and how do you structure post-BAV surveillance?
Q. How should resource availability influence the role of BAV across different healthcare systems?
General cardiologists should be aware of structural interventions, as this represents an entirely new and expanding field that is changing how we manage patients with valvular and structural heart disease. Cardiologists are no longer simply referring these patients to cardiac surgeons; instead, we now play an active role in their treatment and overall care. Visit https://www.csi-congress.org/ to learn more about catheter & structural intervention.
![]() InRhythm is our new, expert-led, practice pearls series delivering concise, actionable insights from leading experts in cardiology. Designed to help healthcare professionals stay current, it highlights real-world challenges, emerging evidence, and actionable strategies to enhance clinical practice, strengthen decision-making, and build confidence in an increasingly complex and fast-evolving field.
InRhythm is our new, expert-led, practice pearls series delivering concise, actionable insights from leading experts in cardiology. Designed to help healthcare professionals stay current, it highlights real-world challenges, emerging evidence, and actionable strategies to enhance clinical practice, strengthen decision-making, and build confidence in an increasingly complex and fast-evolving field.
More content in interventional cardiology.
Cite: Optimizing the role of balloon aortic valvuloplasty in the TAVI era. touchCARDIO. 2 April 2026.
Editor: Victoria Smith, Senior Content Editor.
Disclosures: This article was created by the touchCARDIO team in collaboration with Dr Gustavo Samaja. Views expressed are the speaker’s own and do not necessarily reflect the views of Touch Medical Media.
touchCARDIO utilize AI as an editorial tool (ChatGPT (GPT-4o) [Large language model]. https://chat.openai.com/chat.) The content was developed and edited by human editors. No funding was received in the publication of this article.
Related content:

SIGN UP to touchCARDIOLOGY!
Join our global community today for access to thousands of peer-reviewed articles, expert insights and learn-on-the-go education across 150+ specialties, plus concise email updates and newsletters so you never miss out.











