
Heart failure (HF) is a global health burden, with a 2019 prevalence of 711.90 per 100,000 population, totalling 56.19 million cases and 5.05 million years lived with disability, despite only modest declines since 1990.1 Recent years have shown an uptick in prevalence, driven by ageing populations and improved diagnostics, with disparities persisting between high- and low-sociodemographic index regions.1 HF severely diminishes quality of life (QoL), causing dyspnoea, fatigue and reduced life expectancy.2 Traditional self-management faces challenges such as complex regimens, cognitive impairments and socioeconomic barriers that limit adherence and access to care.3 Telemedicine offers transformative potential by bridging care gaps, reducing costs and enabling remote monitoring, particularly for underserved populations.4 Its efficiency and versatility across medical specialities position telemedicine as a critical tool for addressing systemic barriers and improving HF outcomes.5
The effectiveness of telemedicine in HF self-management is underpinned by several interconnected behavioural and health theories. Self-efficacy theory posits that telemedicine enhances patients’ confidence in managing their condition by providing real-time feedback, continuous symptom monitoring and access to educational tools, thus empowering proactive self-management.6 Building on this, the Health Belief Model explains how telemedicine mitigates perceived barriers (e.g. transportation), highlights the benefits of adherence and reinforces self-efficacy, thereby encouraging behaviour change.7 The chronic care model further supports this by advocating for proactive, patient-centred care through personalized care plans, goal-setting and on-going clinical support.8 The theory of planned behaviour demonstrates that telemedicine may strengthen behavioural intentions by positively influencing attitudes, perceived social norms and the sense of control over health behaviours.9 Similarly, social cognitive theory emphasizes that virtual interactions within telemedicine platforms facilitate observational learning and reinforcement, which are critical for sustaining long-term behaviour change.10 Additionally, the Behavior Change Technique framework highlights how components such as goal-setting and positive reinforcement integrated into telemedicine platforms promote adherence and persistence in self-care behaviours.11 In particular, telephone-based telemedicine offers an immediate and practical form of two-way communication, supporting real-time symptom assessment, patient education and coordination of care, thereby enhancing accessibility and continuity of care in the management of HF.12
Telemedicine for HF management faces challenges, including disparities in technology accessibility, patient engagement and digital literacy, which are often compounded by socioeconomic inequalities.13 Previous systematic reviews have demonstrated telemedicine’s potential to reduce hospitalizations and mortality but have largely overlooked critical barriers to implementation, such as engagement strategies and addressing digital literacy gaps. These studies often lack a comprehensive synthesis of how telemedicine systems can tackle these challenges in diverse healthcare settings.14 This systematic review evaluates clinical outcomes and broader dimensions such as knowledge, QoL and barriers to adoption. It provides actionable insights for addressing barriers and standardizing telemedicine practices by synthesizing evidence across these aspects. Unlike previous reviews that primarily focused on clinical endpoints such as hospitalization and mortality reduction, this review adopts a broader evaluative framework by integrating implementation science perspectives – specifically targeting barriers to adoption such as digital literacy, patient engagement and sociotechnological disparities.15,16 This approach provides a more comprehensive analysis of telemedicine’s real-world effectiveness in HF management, offering new insights into how telehealth platforms can be optimized for diverse patient populations and healthcare systems.17
Methods
Study design and inclusion criteria
This meta-analysis was conducted adhering to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines.18 This systematic review protocol was registered on the International Prospective Register of Systematic Reviews (PROSPERO) with registration number CRD42024621079. Our study aimed to explore the effectiveness of mobile-based health monitoring for patients with HF.
Inclusion of studies was assessed using a set of inclusion and exclusion criteria. Studies were eligible if they:
-
were randomized controlled trials (RCTs);
-
included participants aged 18 years or older;
-
used telemedicine interventions (telephone-based communication, telemedical systems, video call) compared with treatment as usual (TAU); and
-
reported outcomes such as all-cause mortality, cardiovascular mortality, HF-related admissions, patient’s QoL or HF knowledge.
After assessing eligibility, studies were manually screened and excluded with the following criteria:
-
pilot studies/protocol studies;
-
review studies;
-
studies not published in English; and
-
inaccessible studies (irretrievable full texts).
Using the stated inclusion and exclusion criteria, five authors (Derren Rampengan, Stevanus Surya, Diski Saisa, Jade Rampengan and Roy Ramadhan) independently evaluated study eligibility. Any disagreements were resolved through discussion.
Literature search and selection
We systematically searched the PubMed, Cochrane Library, EBSCOhost, Epistemonikos, ProQuest and Scopus databases from inception to 25 February 2025 for RCTs published in English comparing telephone-based telemedicine with TAU. Keywords included: (‘Heart Failure’ OR ‘Cardiac Failure’ OR ‘Congestive Heart Failure’ OR ‘Heart Failure Patients’) AND (‘Telephone’ OR ‘Telemedical Systems’ OR ‘eHealth’ OR ‘Telehealth’ OR ‘Telemedicine’ OR ‘Self-Management Monitoring’ OR ‘Remote Patient Monitoring’) AND (‘Treatment as Usual’ OR ‘Standard Care’ OR ‘Conventional Management’) AND (‘All-Cause Mortality’ OR ‘Cardiovascular Mortality’ OR ‘Heart Failure Related Admissions’ OR ‘Quality of Life’ OR ‘HF Knowledge’). An RCT filter was applied if it was available on the database search.
The screening had two phases: initial title and abstract screening to remove irrelevant records, followed by full-text review against the inclusion criteria. Derren Rampengan, Stevanus Surya and Diski Saisa completed both steps independently. Disagreements were adjudicated by a fourth reviewer (Jade Rampengan) to ensure an impartial, consensus-based selection. Reviewers were blinded to each other’s decisions at both steps to reduce bias.
Quality assessment of selected studies
The methodological quality of each eligible study was assessed using the Cochrane Risk of Bias 2 tool. This revised tool evaluates the risk of bias in RCTs across five domains:
-
the randomization process;
-
deviations from intended interventions;
-
missing outcome data;
-
outcome measurement; and
-
selection of the reported result.
Results were recorded in an Excel file (.xlsx) and uploaded to the Risk of Bias Visualization (ROBVIS) website for visualization.18 Three reviewers (Albert Pratama, Ammar Nojaid and Ika N Kadariswantiningsih) independently assessed the studies, and any disagreements were resolved by consensus.
Data extraction
After a comprehensive screening process, studies that met the eligibility and inclusion criteria were included in both the qualitative and quantitative synthesis. The same, previously mentioned, authors extracted data on study characteristics, including the following:
-
author and year of publication;
-
study location;
-
study population details (sample size and age) and population characteristics (number of male participants, New York Heart Association [NYHA] classification and left ventricular ejection fraction [LVEF]);
-
number of patients allocated to intervention and control groups, along with the type of intervention; and
-
follow-up duration.
Regarding outcomes, data were extracted and analysed for all-cause mortality, cardiovascular-related mortality, HF-related knowledge, HF-related hospital admissions and patients’ QoL. Furthermore, the included studies were categorized into three main groups based on the type of intervention implemented to more specifically evaluate the effectiveness of eHealth management:
-
automated telemonitoring and remote management;
-
human-led communication support; and
-
structured education-based eHealth.
This categorization was made based on the similarity of intervention characteristics.
Data synthesis and analysis
Data were analysed using Review Manager version 5.4 (The Cochrane Collaboration, Copenhagen, Denmark). Continuous outcomes were pooled as mean difference (MD) or standardized MD (SMD) with 95% confidence interval (CI) and presented in forest plots. Dichotomous outcomes were pooled as odds ratios (ORs) with 95% CI. Primary analyses used random-effect models regardless of the magnitude or statistical significance of heterogeneity because clinical and methodological diversity was expected across populations, settings and eHealth interventions. Fixed-effect models were applied only as sensitivity analyses to assess robustness. Statistical heterogeneity was summarized using I² and classified using Cochrane bands: not important (0–40%), moderate (30–60%), substantial (50–90%) and considerable (75–100%). Small study effects and publication bias were assessed by visual inspection of funnel plots when at least 10 studies were available.
Results
Study selection and identification
Database searches yielded 722 potentially relevant records (Figure 1). Of these, 18 articles were excluded as duplicate records. After duplicates were removed, we excluded 303 articles because of irrelevant titles/abstracts, and 401 were reviewed for full text. Finally, 37 RCTs were evaluated in this systematic review and meta-analysis.
Figure 1: PRISMA flowchart
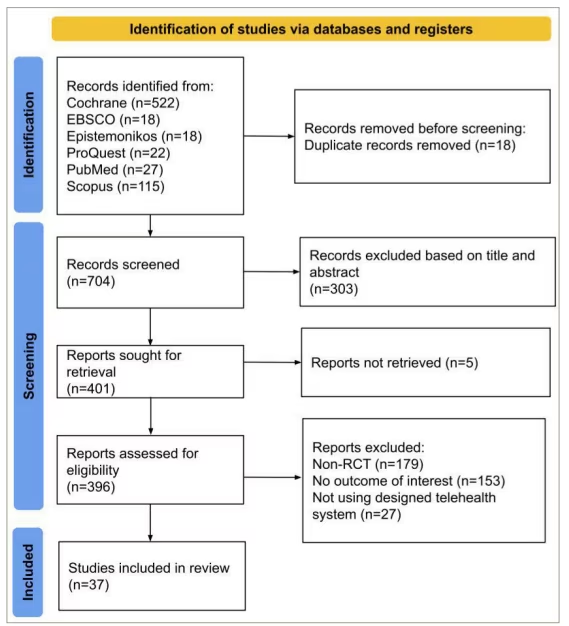
PRISMA = Preferred Reporting Items for Systematic Reviews and Meta-Analyses; RCT = randomized controlled trial.
Characteristics of included studies
All eligible RCTs included in this systematic review are summarized in Table 1.17–54 The review encompasses studies conducted between 2005 and 2024, comprising a total of 37 RCTs involving 13,366 patients with HF from North America, South America, Europe, Asia and Australia. The participants’ mean age ranged from 53.5 to 80.12 years, with a predominantly male population. Most patients were classified as NYHA class II or III. The mean LVEF ranged from 24.66% to 48.4%. Across all studies, 6,585 patients received telemedicine interventions: specifically, 2,452 received automated telemonitoring and/or remote management, 2,668 received human-led communication support and 1,465 participated in structured education-based eHealth programmes. The follow-up duration varied among studies, ranging from 3 to 57 months.
Table 1: Characteristics of included studies17–53
| Author, year | Location | Total patients | Male (%) | Mean age (SD) | Mean LVEF% (SD) | NYHA class | Allocated patients (I/C) | Type of intervention | Follow-up (month) |
| Automated telemonitoring and/or remote management | |||||||||
| Boyne et al. 201217 | The Netherlands | 382 | 59.16 | 71.1 (10.37) | 36.09 (3.4) | II–IV | 197/185 | Telemonitoring device with preset symptoms, knowledge and behaviour dialogues + HF nurse telephone contact if needed | 12 |
| Brugts et al. 202318 | The Netherlands | 348 | 75.58 | 69.38 (2.64) | 30.16 (3.55) | NA | 176/172 | CardioMEMS: Daily remote monitoring of pulmonary artery pressure using the CardioMEMS HF System, with HF therapy (especially diuretics, vasodilators and GDMT) individually adjusted based on the pressure readings | 12 |
| Chaudhry et al. 201029 | USA | 1,653 | 57.96 | 61.02 (3.27) | ≤40 | I–IV | 826/827 | Daily toll-free calls with general health and HF symptoms check via phone keypad; monthly depression screening included | 6 |
| Cichosz et al. 201940 | Denmark | 193 | 80.83 | 70.41 (2.63) | 30.15 (3.55) | II–IV | 93/100 | Daily telemonitoring of vital parameters (BP, HR, weight) and answered daily disease-specific e-questionnaire on a mobile phone. Nurse/physician follow-up if needed | 12 |
| Cleland et al. 2005a48 | Germany, the Netherlands and UK | 253 | 84.98 | 67.34 (12.07) | 24.66 (8) | I–IV | 168/85 | Telemonitoring of vital signs (BP, HR, heart rhythm, weight), twice daily + nurse telephone contact if needed | 8 |
| Dendale et al. 201249 | Belgium | 160 | 65 | 76 (10) | 35 (15) | NA | 80/80 | Usual care + telemonitoring of vital signs. GP will receive an email alert if pre‐defined limits of vital signs were exceeded | 6 |
| Ding et al. 202050 | Australia | 184 | 76.63 | 70.16 (12.33) | 28.24 (12.35) | NA | 91/93 | ITEC-CHF: Remote weight monitoring, structured telephone support and nurse-led care. Rapid weight changes triggered nurse follow-up and HF action plan activation (e.g. GP visit, HF clinic or ED visit) | 6 |
| Dorsch et al. 202151 | USA | 83 | 65.06 | 61.09 (8.99) | 38 (19.41) | I–IV | 42/41 | Mobile-based daily self-monitoring app, ManageHF4Life, along with a Fitbit app for physical activity monitor (Fitbit Charge 2) and health scale (Fitbit Aria and Aria 2) | 3 |
| Galinier et al. 202052 | France | 937 | 72.25 | 69.85 (12.44) | NA | I–IV | 482/455 | Daily body weight measurement and symptom questionnaire via electronic devices with automated alerts. Nurses contacted patients to validate alerts and provide follow-up as needed | 18 |
| Hale et al. 201653 | USA | 25 | 64 | 71.7 (11.2) | NA | I–IV | 11/14 | MedSentry system: An electronic device that alerts patients to take medications, combined with a monitoring centre where advisors contact patients and caregivers if doses are missed | 3 |
| Hindricks et al. 201419 | Australia, Europe and Israel | 664 | 80.72 | 65.55 (9.45) | 26 (6.51) | II–III | 333/331 | Daily automatic implant-based telemonitoring via ICDs or CRT-Ds of heart rhythm parameters, including ventricular and atrial tachyarrhythmias, biventricular pacing percentage, patient activity and ventricular extrasystoles | 11.2 |
| Johnson et al. 202220 | USA | 31 | 58.06 | 58.79 (15.34) | ≤40 | NA | 16/15 | HF-SMART programme: A secure mobile app offering tailored HF education, daily prompts, alerts for urgent issues, nurse-led active monitoring of patient data, interactive symptom feedback with biometric tracking and medication reminders | 3 |
| Kashem et al. 200721 | USA | 48 | 72.92 | 53.5 (10.41) | 25.5 (3.01) | II–IV | 24/24 | Website-based daily telemonitoring of several parameters (BP, HR, weight, steps/day, symptoms) + HF nurse internet-based text messaging if needed | 12 |
| Koehler et al. 201122 | Germany | 710 | 81.27 | 66.9 (10.64) | 26.5 (5.82) | II–III | 354/356 | Physician-led RTM: Daily telemonitoring of heart rhythm, BP and body weight + physician telephone contact to verify measurements, to give consultation or to institute treatment | 26 |
| Konstam et al. 201123 | USA | 88 | 63.64 | 69.3 (12.71) | 30.58 (17.42) | II–IV | 44/44 | AHM: Combined objective monitoring of body weight and vital signs with daily text-based symptoms (dyspnoea, fatigue and oedema) and adherence assessments, included medication review and automated dosing reminders | NA |
| Pekmezaris et al. 201824 | USA | 104 | 58.65 | 59.9 (15.1) | NA | I–III | 46/58 | Daily telemonitoring of vital signs (BP, oxygen saturation, weight and HF) + scheduled weekly video consultations to assess vital signs, discuss symptoms and contribute behaviours, as well as treatment adjustment if required | 3 |
| Sahlin et al. 202225 | Sweden | 118 | 60.17 | 79 (10) | NA | I–IV | 58/60 | Home-based self-care tool (OPTILOGG): Daily telemonitoring of weight tracking, symptom assessment, interactive education and loop diuretic dose adjustments. Patients also engage in short, structured educational modules on HF self-care | 8 |
| Scherr et al. 200926 | Austria | 108 | 76.7 | 66.13 (2.44) | 27.3 (3.98) | II–IV | 54/54 | Daily telemonitoring of vital parameters (BP, HR, body weight) and their dosage of HF medication + telephone contact if needed | 6 |
| Seto et al. 201227 | Canada | 100 | 79 | 53.7 (13.7) | 27.05 (8.87) | II–IV | 50/50 | Daily telemonitoring of vital parameters (BP, HR, body weight), weekly single-lead ECGs and answered daily symptom questions on a mobile phone + telephone contact (if necessary) | 6 |
| Wagenaar et al. 2019a28 | The Netherlands | 300 | 74 | 66.75 (11.29) | NA | I–IV | 150/150 | EACP: EACP group received the same HFM website guidance plus access to the e-Vita platform for daily or personalized monitoring of weight, BP and HR, with nurse phone follow-up for symptom assessment and care adjustment | 12 |
| Human-led communication support | |||||||||
| Antonicelli et al. 200830 | Italy | 57 | 61.40 | 78.02 (7.06) | 48.4 | II–IV | 28/29 | Weekly phone contact to assess symptoms, treatment adherence, BP, HR, weight, 24-hour urine output and ECG transmission | 12 |
| Cleland et al. 2005b48 | Germany, the Netherlands and UK | 258 | 82.17 | 67.33 (10.67) | 24.67 (8) | I–IV | 173/85 | NTS: Monthly calls by HF nurse to assess symptoms and medications; patients could contact the nurse anytime | 8 |
| Domingues et al. 201031 | Brazil | 111 | 68 | 63 (13) | 29 (8) | NA | 48/63 | Nurse follow-up: Eight scheduled calls over 3 months (weekly in month 1, biweekly in months 2–3), starting 7 days post-discharge to reinforce instructions, monitor decompensation and assess ER visits or rehospitalizations | 3 |
| Dunagan et al. 200532 | USA | 151 | 56.29 | 69.95 (13.28) | NA | II–IV | 76/75 | Scheduled nurse-led telephone-based education and monitoring (supervised by HF cardiologists) to promote self-management, appropriate diet, therapy adherence and screen for HF exacerbations | 12 |
| Ferrante et al. 201033 | Argentina | 1,518 | 70.8 | 65 (13.3) | NA | III–IV | 760/758 | Patients received an explanatory booklet and biweekly calls by specialized nurses, with call frequency adjusted after the fourth call based on case severity and compliance | 57 |
| GESICA Investigators 200534 | Argentina | 1,518 | 70.8 | 65 (13.3) | NA | III–IV | 760/758 | Nurse-led telephone follow-up: Patients received an education booklet and regular standardized calls to educate and monitor diet, medication adherence, symptoms, fluid retention and activity; nurses adjusted diuretics or recommended additional medical visits as needed | 16 |
| Giordano et al. 200835 | Italy | 460 | 93.48 | 57 (10.04) | 27 (7.58) | II–IV | 230/230 | HBT: Weekly or biweekly scheduled calls (based on NYHA class). Nurses conducted a structured interview to assess clinical condition, fluid and sodium intake, medication adherence, BP and weight. ECG transmission was requested if needed | 12 |
| Krum et al. 201336 | Australia | 405 | 63.21 | 73 (10.54) | 35.97 (19.71) | II–IV | 188/217 | Usual care + intervention: Monthly structured calls to assess HF clinical status, medical management and social factors; 24 h dial-in system for symptom advice and referral to GP or emergency care as needed | 12 |
| Krzesinski et al. 202237 | Poland | 603 | 79 | 67 (14) | 32 (15) | I–IV | 298/305 | AMULET model: Out-patient nurse-led telecare involving symptom questionnaires to assess the presence and severity of HF symptoms, along with impedance cardiography and a bioimpedance scale to evaluate HF status; results are reviewed by a physician to provide patient-specific recommendations | 12 |
| Nomali et al. 202438 | Iran | 68 | 70.59 | 55 (13.6) | ≤40 | II–IV | 34/34 | Face-to-face HF self-care education by nurses, daily home self-monitoring of body weight and dyspnoea using a paper-based coloured diary and scheduled nurse follow-up calls | 3 |
| Shearer et al. 200739 | USA | 87 | 64.4 | 76.03 (8.32) | 34.5 (15.3) | I–IV | 42/45 | Usual care + intervention: Telephone-delivered EI that provides them support and information designed to focus specifically on what was important to the patient in self-management, goal attainment and functional health | 6 |
| Wallström et al. 201941 | Sweden | 77 | 63.36 | 80.12 (9.67) | NA | NA | 39/38 | PCC in the form of structured telephone support for 6 months, aims to explore the participants’ wishes, abilities, problem areas and formulated reachable goals | 6 |
| Yu et al. 201542 | China | 160 | 65.63 | 59.35 (10.78) | 40.06 (15.23) | II–IV | 80/80 | Health education booklet on HF basics and self-management + telephone follow-ups to monitor adherence to medication and lifestyle changes | 3 |
| Structured education-based eHealth | |||||||||
| Clays et al. 202143 | Belgium and Italy | 56 | 77 | 63 (10.5) | 32.2 (6.3) | II–III | 34/22 | HeartMan mobile personal health system: Daily telemonitoring with DSS-guided support for physical health (vitals, exercise, lifestyle advice on nutrition, medication reminders and self-monitoring), psychological support (CBT, mindfulness exercise) and HF education | 6 |
| Koehler et al. 201844 | Germany | 1,538 | 69.57 | 70 (10.51) | 41 (13) | I–IV | 765/773 | Secure web-based system for daily monitoring of BP, body weight, HR, heart rhythm, SpO2 and self-rated health daily; HF education; monthly structured nurse phone interviews assessing clinical status, symptoms, medications and adherence | 12 |
| Lakdizaji et al. 201345 | Iran | 44 | 56.82 | 61.7 (9.46) | ≤40 | II–III | 22/22 | Three-month on-going educational programme: one-on-one teaching, educational booklet based on Heart Failure Society of America modules (covering disease control, diet, medications, physical activity and self-care), home visits every 3 weeks and follow-up phone calls | 3 |
| Piotrowicz et al. 201946 | Poland | 850 | 88.59 | 62.4 (10.5) | 30.5 (7.01) | I–III | 425/425 | HCTR programme: A 9-week programme with a 1-week in-hospital phase for assessment, treatment optimization, education and exercise planning, followed by 8 weeks of home-based HCTR (five sessions/week) | 26 |
| Riegel et al. 200647 | USA | 134 | 46.3 | 72 (11) | 43.2 (18.1) | III–IV | 69/65 | TCM: Structured calls to assess HF hospitalization risk (e.g. poor adherence), teach self-care (symptom and diet management) and provide culturally tailored education focused on personalized care, family involvement and trust | 6 |
| Wagenaar et al. 2019b28 | The Netherlands | 300 | 73.67 | 66.8 (10.99) | NA | I–IV | 150/150 | HFM website: Patients received usual care plus access to the HeartFailureMatters.org website, a key information leaflet, quarterly email reminders and follow-up discussions on website use | 12 |
AHM = Automated Home Monitoring; AMULET = A Model of Up-to-date Leading Telecare; BP = blood pressure; CBT = Cognitive Behavioural Therapy; CRT-Ds = Cardiac Resynchronization Therapy Defibrillators; DSS = Decision Support System; EACP = eHealth-Adjusted Care Pathway; ECG = electrocardiogram; ED = Emergency Department; EI = empowerment intervention; ER = emergency room; GDMT = Guideline-Directed Medical Therapy; GP = general practitioner; HBT = home-based telemanagement; HCTR = Hybrid Comprehensive Telerehabilitation; HF = heart failure; HFM website = Heart Failure Matters Website; HR = heart rate; I/C = Intervention/Control groups; ICDs = Implantable Cardioverter-Defibrillators; ITEC-CHF = Innovative Telemonitoring Enhanced Care for Chronic Heart Failure; LVEF = left ventricular ejection fraction; NA = not available; NTS = Nurse Telephone Support; NYHA = New York Heart Association; PCC = patient-centred care; RTM = remote telemedical management; SD = standard deviation; SpO2 = peripheral oxygen saturation; TCM = telephone case management.
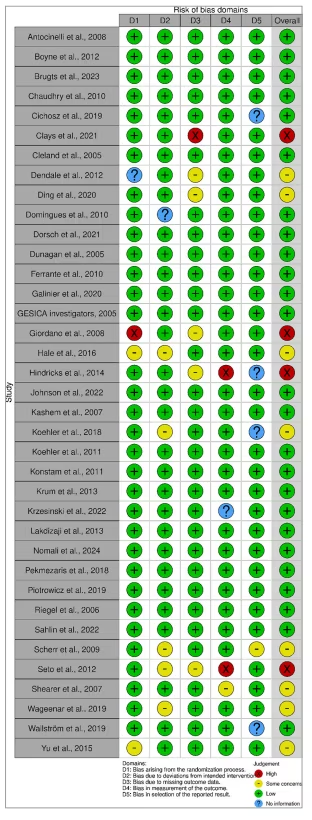
The overall risk of bias, as shown in the summary graph, indicated a low risk across the five assessment parameters (Figure 2). Specifically, our appraisal shows that twenty-five studies were at low risk of bias, eight studies had some concerns, which is especially due to the lack of details regarding the randomization process and some studies were judged to have moderate attrition in deviations and data management, which raises uncertainty on the bias, and four studies were at high risk of bias due to the non-blinding of participants, considering the nature of the intervention, some using patient-reported outcomes and no adequate methods in handling missing data (Figure 3).17–53
Figure 2: Risk of bias summary using the Cochrane Risk of Bias 2.0 tool for randomized controlled trial studies
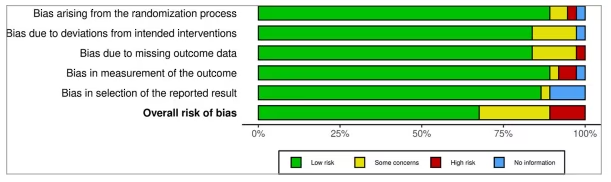
Figure 3: Risk of bias quality assessment graph using traffic-light plot17–53
Meta-analysis of eHealth interventions in population with heart failure
Cardiovascular mortality
Nine studies investigated the effect of telemedicine on cardiovascular mortality outcomes (Figure 4).18,22,28,31,35,37,44,46,52 Analysis showed that cardiovascular mortality was not reduced by the use of telemedicine (OR: 0.85 [95% CI: 0.71, 1.01; p=0.07]). The funnel plot showed a symmetrical distribution with minimal outliers, suggesting non-significant heterogeneity and low risk of publication bias among included studies (Figure S1). True heterogeneity across the studies was not significant (I2=0%). Subgroup analysis showed that automated telemonitoring, human-led communication support and structured education-based eHealth had no significant result in cardiovascular mortality.
Figure 4: Forest plot of eHealth systems’ impact on cardiovascular mortality in patients with HF18,22,28,31,35,37,44,46,52
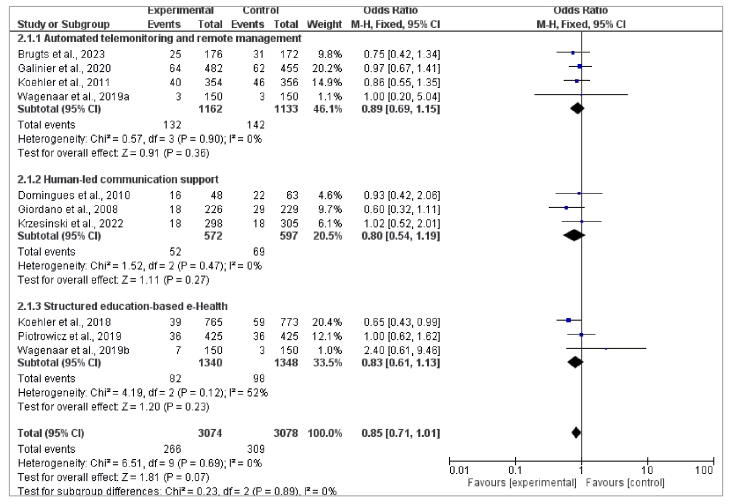
CI = confidence interval; HF = heart failure; MH = Mantel-Haenszel method.
All-cause mortality
Twenty-five studies reported all-cause mortality, and the results can be seen in Figure 5.17–22,25–37,41,44,46,48,49,52 Meta-analysis showed that the telemedicine group insignificantly changed all-cause mortality (OR: 0.93 [95% CI: 0.85, 1.03; p=0.16]). Heterogeneity was found to be not significant (I2=24%), and the funnel plot also showed a few outliers, indicating evidence of true heterogeneity among studies (Figure S2). Subgroup analysis revealed that human-led communication support showed the highest incidence of all-cause mortality, but all groups showed non-significant results (p=0.52).
Figure 5: Forest plot of eHealth systems’ impact on all-cause mortality in patients with HF17–22,25–37,41,44,46,48,49,52
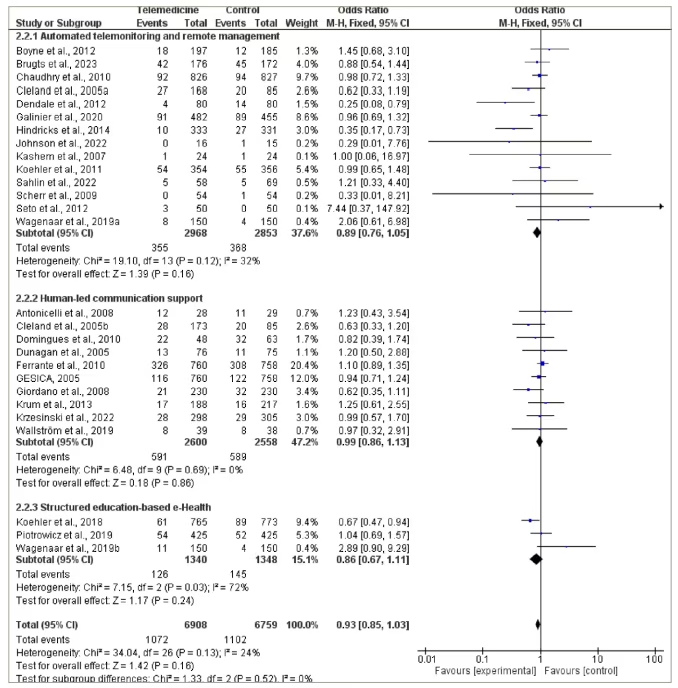
CI = confidence interval; HF = heart failure; MH = Mantel-Haenszel method.
Quality of life
Eight trials were included to evaluate the QoL score. The Minnesota Living with Heart Failure Questionnaire (MLHFQ) score was used to evaluate QoL. Pooled analysis is shown in Figure 6.23,27,32,42–45,47 There is no significant difference in QoL between the two groups on subgroup analysis for physical domain (MD: -4.34 [95% CI: -8.97, 0.29; p=0.07]) (Figure 6A), emotional domain (MD: -2.40 [95% CI: -5.75, 0.95; p=0.16]) (Figure 6B) and total domain (MD: -7.25 [95% CI: -14.81, 0.31; p=0.06]) (Figure 6C). The degree of heterogeneity was considerable (I2=91%).
Figure 6: Forest plot of eHealth systems’ impact on QoL in patients with HF23,27,32,42–45,47
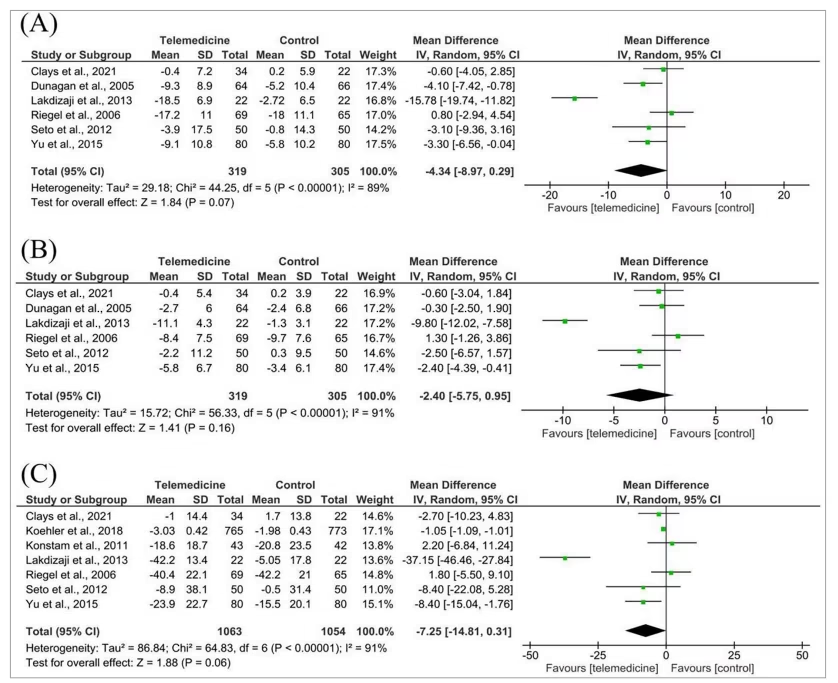
QoL based on the MLHFQ questionnaire: (A) physical dimension, (B) emotional dimension and (C) overall dimension.
CI = confidence interval; HF = heart failure; IV = inverse variance; MLHFQ = Minnesota Living with Heart Failure Questionnaire; SD = standard deviation; QoL = quality of life.
Heart failure-related knowledge
Five studies evaluated the effect of telemedicine on HF-related knowledge (Figure 7).23,24,38–40 The overall effect was not significant (SMD: 0.53 [95% CI: -0.12, 1.19; p=0.11]). True heterogeneity across the studies was found to be considerable (I2=92%). Automated telemonitoring showed higher knowledge scores compared with human-led communication support (SMD: 1.00 versus 0.26, respectively), but the difference was not statistically significant.
Figure 7: Forest plot of eHealth systems’ impact on HF-related knowledge in patients with HF23,24,38–40
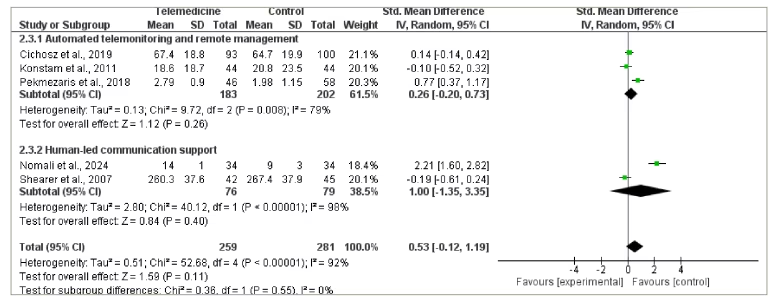
CI = confidence interval; HF = heart failure; IV = inverse variance; SD = standard deviation; Std. = standardized.
Heart failure-related admission
Twenty-two studies reported HF-related admission. Figure 8 showed that the telemedicine group is favourable with an OR of 0.73 (95% CI: 0.62, 0.86; p=0.0002), and the p-value revealed that the result is statistically significant.17,18,21,22,25,28,29,32–37,41,46,48,50–53 Heterogeneity was found to be substantial (I2=61%). In subgroup analysis, we found significant results in the human-led communication support group (OR: 0.67 [95% CI: 0.59, 0.77; p<0.00001]). Automated telemonitoring and structured education-based eHealth showed no differences in HF-related admission incidence between the telemedicine and control groups. The funnel plot shows no evidence of true heterogeneity among studies (Figure S3).
Figure 8: Forest plot of eHealth systems’ impact on HF-related admission in patients with HF17,18,21,22,25,28,29,32–37,41,46,48,50–53
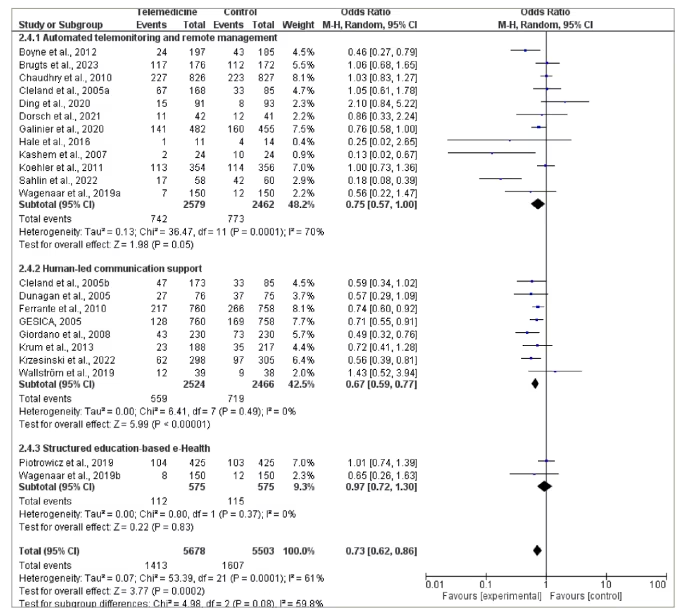
CI = confidence interval; HF = heart failure; MH = Mantel-Haenszel method.
Discussion
Overview of findings
The present systematic review and meta-analysis showed a significant reduction in HF-related admission, though it was moderately heterogeneous in the pooled results. Despite two studies – Ding et al. and Wallstrom et al. – reporting results that contradicted the overall trend, their impact on the pooled analysis was minimal due to the relatively small number of cases included.41,50 However, no significant difference was found in terms of QoL, cardiovascular mortality, all-cause mortality and HF-related knowledge between the telemedicine and control groups.
Heart failure-related hospitalizations and readmissions
In terms of HF-related admissions, some outliers, such as Dendale et al. and Seto et al., reported smaller or negligible effects, diverging from the overall trend.27,49 However, our pool analysis is supported by studies demonstrating significant benefit. A Model of Up-to-date Leading Telecare (AMULET) study by Krzesinski et al. reported a significant 31% reduction in unplanned HF hospitalizations or cardiovascular death over 12 months.37 Similarly, Chow et al. demonstrated that telemonitoring resulted in a 38% reduction in all-cause readmissions within 180 days and a 68% reduction in 1-year all-cause mortality, highlighting a substantial survival benefit from remote monitoring.54 These findings, which reflect comparable effect sizes, reinforce the potential efficacy of telemedicine interventions in improving clinical outcomes and reducing hospital burden in similar patient populations.
Economic impact and cost-effectiveness
Many patients with chronic HF suffer from worsened health status, leading to hospitalization, representing a major component of the economic burden. A pre–post-trial on telemonitoring demonstrated a significant 70% reduction in the number of patients experiencing at least one hospitalization due to HF, along with a clinically meaningful 49% reduction in hospitalization-related costs – from €2,189 with standard care to €1,114 with telemonitoring – over a 6-month period.55 Moreover, the Danish TeleCare North trial (Telemedicine for Patients Suffering From COPD; ClinicalTrials.gov identifier: NCT01984840) revealed a positive incremental net monetary benefit of £5,164 and a statistically significant 35% reduction in overall healthcare costs over 1 year.56 Similarly, a Markov model evaluating a hypothetical cohort of older patients with HF in Hong Kong during the coronavirus disease 2019 (COVID-19) pandemic demonstrated that telemonitoring combined with standard care yielded an incremental cost-effectiveness ratio of only US$4,292 per quality-adjusted life year (QALY) gained, well below the willingness-to-pay threshold of US$48,937 per QALY. No threshold was identified in the deterministic sensitivity analysis, and the intervention was considered cost-effective in 99.22% of 10,000 Monte Carlo simulations in the probabilistic sensitivity analysis, indicating a high likelihood of economic favourability for the telemonitoring strategy.57
Quality of life and instrument constraints
Insignificant results in the quality-of-life variable may be attributed to the high heterogeneity of the results. Specifically, Riegel et al. reported a better QoL in all aspects in the control group compared with the telemedicine group, in which these findings are contradictory to other studies.47 This variability probably contributed to differences in sample size, patient characteristics, intervention protocols and follow-up durations. In addition, these findings might have been influenced by limitations of the MLHFQ itself, which include its limited ability to capture all relevant aspects of HF-related QoL, possible recall bias related to the 4-week recall period and potential mistakes caused by inconsistent administration or misinterpretation of questionnaire items.58
Patient knowledge outcomes
For HF-related knowledge, the non-significant pooled outcome may be partially attributed to the study by Nomali et al., which reported an exceptionally large effect size in favour of telemedicine, accompanied by wide CIs and low statistical weight.38 This combination indicates high variability and suggests that the study may have exerted a disproportionate influence on the pooled estimate, thereby contributing to the observed heterogeneity in the analysis.
Mortality results and comorbidity effects
Results cannot be attributed to another study; likely, the authors mean that they may be explained by the findings of Galinier et al., which reported no significant effect despite accounting for over 20% of the total weight in this outcome, thereby reducing the influence of smaller studies that showed potential benefits.52 The insignificant result in all-cause mortality variable was mainly caused by the contradictory results of Ferrante et al., with a relatively high analysed weight because of their high number of cases.33 This aligns with other studies, such as Koehler et al. and Krzesinski et al., which showed less pronounced or negligible reductions in mortality.37,44 In contrast, Brugts et al. and Chow et al. demonstrated that eHealth interventions significantly reduced all-cause mortality.18,54
Comparison with previous evidence
Our findings are in accordance with a prior review by Rebolledo et al., which demonstrated a statistically significant decreased risk of HF hospitalization, while there is a non-statistically significant decrease in cardiovascular mortality and all-cause mortality.59 While evidence supporting reduced HF hospitalization outcome remains consistent across multiple reviews, the findings on mortality outcome were heterogeneous.17,60–64 Several reviews found that eHealth interventions had significant reductions in mortality, whereas others found contradictory results.17,60–66 This inconsistency reflects variability across study design and may also reflect patient-level factors, such as the high multimorbidity burden in the older population with HF. Large registry data show that 55–98% of adults ≥60 have two or more chronic diseases.67 Fatal events or exacerbations attributable to non-HF comorbidities (e.g. chronic kidney disease, chronic obstructive pulmonary disease, stroke, anaemia, sepsis) may not be intercepted by HF-specific telemonitoring algorithms, diluting observable mortality effects. Future studies should incorporate multi-condition monitoring and stratify analyses by comorbidity load to clarify true survival impact.
Previously, a network meta-analysis reported that telemedicine interventions significantly reduced HbA1c compared with standard treatment.68 In another meta-analysis, telemedicine was found to be more effective in decreasing HbA1c than standard care alone.69 A meta-analysis of four clinical studies indicated that telemedicine for patients with gestational diabetes mellitus resulted in a notable reduction in unplanned clinical visits.70 These data from previous literature indicate that telemedicine has a potential role in diabetes care, consistent with the results from the present studies. Implementing telemedicine is highly feasible, as suggested by a previous study on hypertension therapy.71 The telemedicine allows blood pressure monitoring and provides medical practitioners with remote access.71 Throughout the COVID-19 pandemic, it was employed more often to provide continuity of care and improve access to medical services.72,73 Patients with chronic renal disease exhibiting resistant hypertension have demonstrated improvement with a collaborative eHealth system involving both nephrologists and pharmacists.74 By reducing healthcare access barriers, improving clinical outcomes and extending services to remote areas, telemedicine proves to be an effective tool in chronic disease management.75
Mechanistic links and behaviour change
Findings from the present study have also important implications for behavioural change theories, particularly those highlighted in the Health Belief Model and the theory of planned behaviour.7,8,76 Telemedical interventions enhance patients’ understanding of their disease, addressing ‘perceived severity’ and ‘perceived susceptibility’ as outlined in the Health Belief Model, thereby promoting better self-management. Similarly, the regular monitoring and feedback provided by telemedicine empower patients with a stronger sense of control over their health, which aligns with the theory of planned behaviour’s concept of perceived behavioural control.7 By fostering self-efficacy and enhancing collaboration between patients and providers, telemedicine likely contributes to reductions in hospitalizations, supporting the principles of the social cognitive theory.
Limitations and future directions
Our study contributes to the growing body of evidence on the benefits of telemedicine in healthcare, specifically in patients with HF, among others. Further research is required on suitable specific telemedicine methods for improving QoL and HF-related knowledge and reducing cardiovascular and all-cause mortality in patients with HF, for which our study showed insignificant results. We further acknowledge the limitations of the present study, which warrant its cautious interpretation. The included studies exhibited variability in the types of telemedicine interventions, their frequency and their integration with standard care, potentially influencing the outcomes and limiting generalizability. Additionally, most studies were conducted in high-income countries, limiting applicability to low- and middle-income settings where eHealth-related infrastructure may differ. Future research should aim to standardize telemedical protocols, include diverse populations and evaluate outcomes over longer follow-up periods.
Conclusion
The present systematic review and meta-analysis suggest that the incorporation of telemedicine into conventional care for HF effectively reduces the HF-related hospitalizations. Nonetheless, eHealth intervention did not significantly improve QoL, cardiovascular mortality, all-cause mortality and HF-related knowledge, despite being potential delivery tools for Health Belief Model and the theory of planned behaviour. We recommend future research in prioritizing the standardization of telemedical procedures, encompassing various populations and assessing long-term results.












