

Persistent atrial fibrillation remains a heterogeneous and complex arrhythmia, with outcomes after ablation varying widely depending on the extent of atrial remodeling. At the European Heart Rhythm Association (EHRA) Congress 2026, Dr Amir Sherwan Jadidi (Head of Arrhythmia and Electrophysiology Division, Cantonal Hospital of Lucerne, Lucerne, Switzerland) presents findings from the SOLVE-AF trial, a multicentre randomized study exploring whether targeting atrial substrate abnormalities in sinus rhythm can improve outcomes beyond pulmonary vein isolation alone. By stratifying patients based on the presence or absence of fibrotic low-voltage areas and abnormal electrograms in sinus rhythm, the study highlights a more individualized approach to ablation—where PVI may suffice in less remodeled atria, but additional substrate modification significantly improves success in advanced disease. These results reinforce the concept that persistent AF is not a uniform entity, and suggest that high-density mapping in sinus rhythm may offer a more precise framework for identifying arrhythmogenic substrates and guiding tailored ablation strategies in routine practice.
Could you provide a brief overview of the SOLVE-AF study and its clinical significance?
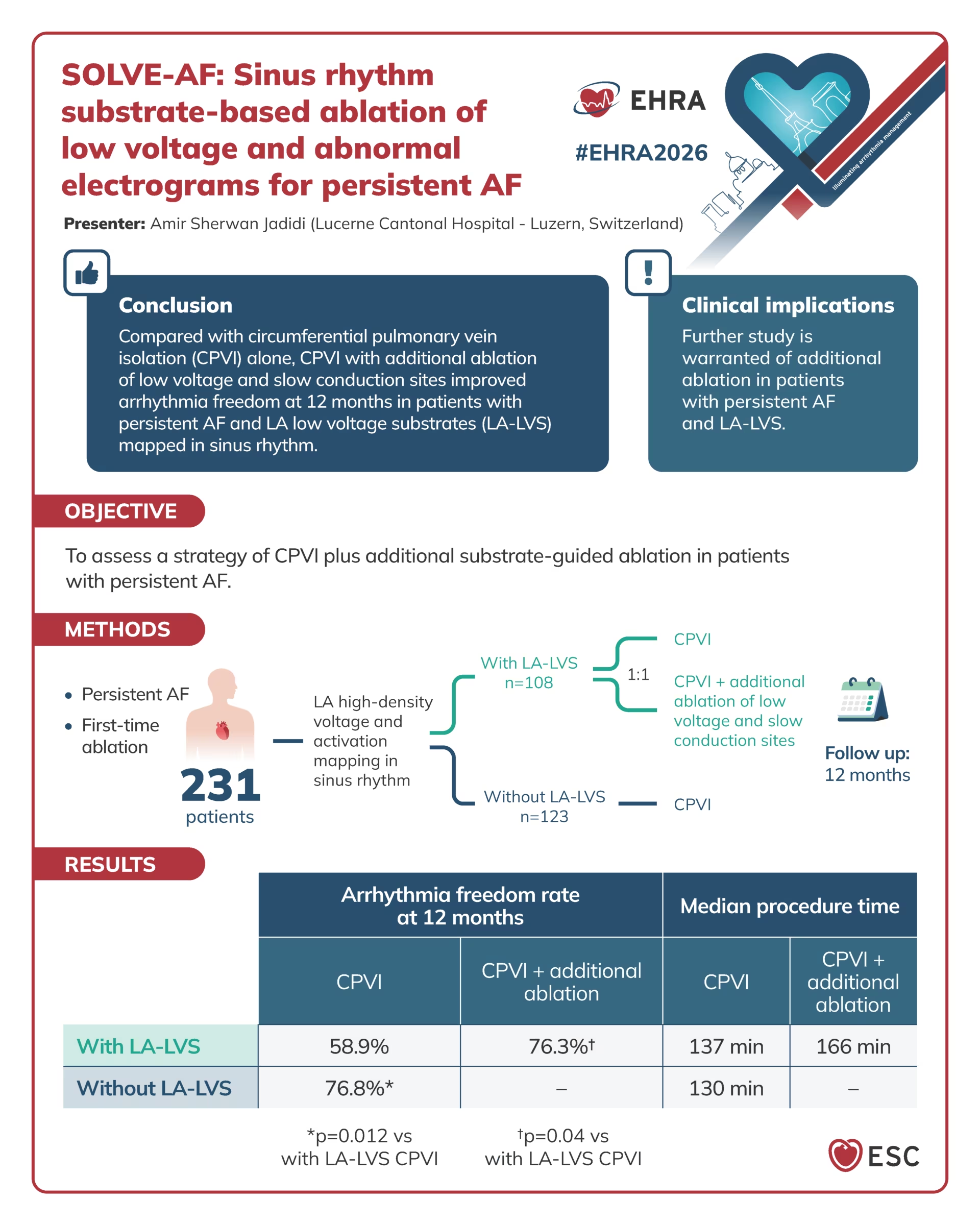
The SOLVE-AF study is multicentric prospective randomized study, assessing the impact of additional sinus rhythm substrate-based ablation in patients with persistent atrial fibrillation (AF) if this novel strategy may improve success rates of ablation therapy and maintain sinus rhythm. Persistent AF goes with different stages of atrial remodeling: in the initial stage, patients have mainly dilated left atria without relevant fibrosis and without fragmented electrograms as evidence for slow conduction sites in the atrium. A smaller portion of persistent AF patients presents a more advanced disease: these are more frequently female patients and patients older than 70 years. In these patients with advanced atrial disease with fibrotic low voltage and slow conduction, the isolation of pulmonary veins does not provide very good results. The study could show that pulmonary vein isolation (PVI) only results in high successes of 76% at 1 year in patients who do not have advanced disease, so patients without fibrotic low voltage areas. In contrast, in patients with advanced disease (with low voltage areas and slow conduction), isolation of pulmonary veins only results in a success rate of 59% at 1 year. However, PVI plus additional catheter ablation of left atrial fibrotic slow conduction areas that are detected with our novel approach during sinus rhythm, improves the success rate in these patients to 76% at 1 year. Especially interesting is that the recurrence of atrial fibrillation is only 11% of 1 year; in other words, 89% of patients do not have AF anymore after this novel approach. So the approach is very promising and for the first time very positive in persistent AF.
How does the Solve AF strategy of substrate-based ablation and sinus rhythm refine our current understanding of atrial fibrillation mechanisms, particularly in patients with persistent AF?
So it shows us that “persistent AF is not equal persistent AF”. We are dealing with different stages of atrial remodeling in persistent AF patients. Development of persistent AF, in contrast to paroxysmal, requires a certain dilation of the left atrium. Patients presenting left atrial dilation but no substantial fibrosis/low voltage areas do respond very well to PVI-only strategy; as a primary catheter ablation strategy, they don’t need ablation of further structures. In contrast, accurate treatment of patients with advanced stage of atrial fibrosis necessitates advanced mapping techniques, which should be done primarily during sinus rhythm, as shown in our study. Mapping and ablation of the areas displaying low voltage, slow conduction with abnormal electrograms improves the success rate in these advanced stages of atrial fibrillation to the same level of 76% as those who have limited remodeling without relevant scar tissue. So basically, a mapping-guided patient-tailored ablation strategy is needed in patients with persistent AF to address the individual’s arrhythmogenic substrate and obtain highest arrhythmia freedom rates/success rates.
How do the outcomes observed in SOLVE-AF compare with prior studies evaluating adjunctive substrate modification, and what might explain differences in efficacy across trials?
Multiple studies have already shown that younger patients (<65 years old) with persistent AF do not have yet advanced stage of fibrosis, they mainly have dilation of left atrium. These studies have shown that in this younger age patient group a PVI-only strategy may reach success rates between 75 and 80%, and this is again confirmed in our study. Our study shows that, in patients with more advanced atrial disease, mapping in sinus rhythm (and not during atrial fibrillation, where we may have some confounding and functional phenomena/wave collision areas) provides clearly interpretable findings and identifies arrhythmogenic slow conduction areas. Notably, ablation of these diseased atrial areas improves success rates and preserves healthy atrial tissue, as only diseased fibrotic/slow conduction areas are targeted by the novel approach.
What are the practical considerations of conducting substrate mapping and ablation in sinus rhythm, and how could this approach shape the standardization of procedures in electrophysiology laboratories?
So the question is: what is necessary to create high density and high-quality sinus rhythm voltage and activation maps revealing the arrhythmogenic atrial sites? We need dedicated high-resolution electro-anatomical mapping using small electrode mapping catheters, as used in the study. Patients need to be first cardioverted to sinus rhythm prior to ablation of the atrial tissue, in order to undergo mapping and analysis of the natural stage of the atria during sinus rhythm. Persistent AF patients who recur shortly after cardioversion to atrial fibrillation should first undergo a circumferential PVI. After PVI, 90-95% of these patients maintain sinus rhythm after electrical cardioversion, allowing to acquire the high-resolution substrate map during sinus rhythm and define the necessary ablation lesion set in case of abnormal sinus rhythm substrate.
Based on the SOLVE-AF findings, how might this strategy influence future research directions or the development of next generation ablation approaches to persistent AF?
We are getting new technologies to make better lesions, to make better and more durable PVI, which will even improve the success rate that we have seen in the SOLVE-AF study with regard to PVI responders. In the SOLVE-AF study, we used point-by-point radiofrequency (RF) ablation, which had a success rate of about 76% in patients without fibrosis and low voltage. With the novel ablation technologies using pulsed field ablation, these results may be even better because the PVI will be more durable and complete. Beyond this, we need new technologies to automatically identify the regions of abnormal electrograms and slow conduction and interpret the atrial signals in an objective way that the SOLVE-AF findings can be reproduced all over the world and not only in a few expert centers. I think these are novelties that will come in the next years; new algorithms to detect those areas of arrhythmogenesis during sinus rhythm and new energy forms that are more effective. Furthermore, novel ablation technologies are needed to treat/ablate more efficiently/durably the fibrotic slow conduction areas that are identified with the novel in sinus rhythm mapping approach.
Visual summary by and provided with kind permission from the European Society of Cardiology.
References
- Jadidi AS. SOLVE-AF: Sinus rhythm Substrate-based ablation Of Low Voltage and abnormal Electrograms for persistent Atrial Fibrillation. Presented at: EHRA 2026, Paris, France, 12 April 2026. Available at: https://esc365.escardio.org/presentation/321185 (accessed 1 May 2026).
Cite: Jadidi AS. SOLVE-AF: Personalizing Substrate Ablation for Persistent Atrial Fibrillation. touchCARDIO. 4 June 2026.
Editor: Heather Hall, Managing Editor
Interviewer: Caroline Markham, Head of Strategic Partnerships
Disclosures: Amir Sherwan Jadidi has no financial or non-financial relationships or activities to declare in relation to this interview. This interview was conducted as part of our coverage of the European Heart Rhythm Association (EHRA) 2026 conference and does not constitute endorsement from EHRA or the ESC. This article was edited by the touchCARDIO team utilizing AI as an editorial tool (ChatGPT (GPT-4o) [Large language model]. https://chat.openai.com/chat.) The content was developed and edited by human editors. Views expressed are the author’s own and do not necessarily reflect the views of Touch Medical Media. No funding was received in the publication of this article.
Related content:

SIGN UP to touchCARDIOLOGY!
Join our global community today for access to thousands of peer-reviewed articles, expert insights and learn-on-the-go education across 150+ specialties, plus concise email updates and newsletters so you never miss out.










