
Coronary artery dissection is a common occurrence during lesion preparation and after drug-coated balloon (DCB) inflation.1 Recent DCB studies focusing on coronary dissections have shown a few key findings:
-
Their angiographic incidence varies between 35 and 60%.
-
Non–flow-limiting dissections left untreated had no correlation with increased risk of target vessel failure (TVF) or late lumen loss.2–7 This reiterates the lessons learnt from the plain old balloon angioplasty (POBA) era that therapeutic dissections, including National Heart, Lung, and Brain Institute (NHLBI) types A, B and uncomplicated type Cs, were not linked to restenosis, and type B has the lowest restenosis rate of all dissection types.
-
Almost 95% of the dissections healed during 6–9 months post-DCB in both angiography and intravascular imaging-guided follow-up.
-
The bailout stenting (BOS) rates due to coronary dissection range from 11 to 21%.2,4–11 The decision to perform BOS for certain degrees of angiographic dissection is operator-dependent, and in the hands of experienced DCB operators, the threshold to stent is higher.4,7 This emphasizes the significant learning curve in perfecting the intricacies of DCB angioplasty.
As an early adopter with over a decade of experience in treating all subsets of coronary lesions with DCB, some of our SPARTAN-Norfolk consortium (long-term safety of paclitaxel drug-coated balloon-only angioplasty for de novo coronary artery disease) operators’ BOS rate is less than 10%, which is low compared with the above studies. The safety and cost-effectiveness of our DCB practice are evident in our published immediate and long-term safety data compared with drug–eluting stent (DES).12–18 Our decision-making criteria, in terms of BOS, evolved over the years as we adopted ways of achieving safe dissections through controlled uniform dilatation during lesion preparation and refined techniques to modify dissections in cases of persistent contrast hang-up or indeterminate angiographic appearances. The key is avoidance, recognition and management (ARM) of a flow–limiting dissection to facilitate a DCB strategy.19 It is crucial to recognize and differentiate a safe, uncomplicated, non-flow-limiting dissection from an unsafe, complicated, flow-limiting category based on a combination of angiographic evaluation of thrombolysis in myocardial infarction (TIMI) flow, residual stenosis, persistence of contrast hang-up, haemodynamic factors and chest pain.1 This suggests that the NHLBI dissection classification is perhaps outdated for current practice. Hence, we put forth a straightforward way of categorizing coronary artery dissections as ‘non-vessel-threatening dissection (non-VTD)/safe to leave/type 1’ and ‘vessel-threatening dissection (VTD)/need to stent/type 2’. We have compiled cases for each category and share our experiences of successfully modifying dissections.
Avoid, recognize and manage dissections
Avoid
A meticulous and cautious preparation of a specific target lesion will minimize the occurrence of a flow-limiting dissection. There are certain patient, angiographic and procedural factors associated with the incidence of dissection. Such factors to be considered include age ≥62, female gender, acute coronary syndromes (ACS), right coronary lesion (RCA), lesion at a bifurcation or a curve, long diffuse disease, eccentric irregular lesions, a larger balloon-to-artery ratio assignment (>1.3:1), higher inflation pressure and multisite dilatation at a tortuosity, as elucidated in our previous article.1 For example, in cases involving lesions localized at curves, bifurcations or tortuosity, a larger balloon size or high-pressure inflations may be avoided. In our practice, we use lower-than-nominal pressure during initial inflation with an appropriately sized semi- or non-compliant balloon (NCB) (1:1 balloon-to-artery size) to achieve adequate balloon expansion, thereby reducing vessel trauma and the potential for a VTD.19 If either full balloon expansion failure occurs or subsequent recoil is seen, we transition to a higher-pressure NCB or a scoring or cutting balloon, especially in calcified lesions. This causes longitudinal controlled dissections rather than uncontrolled VTD. Downsizing the cutting balloon by 0.5 mm may also be used to limit such dissections, which is a widely accepted practice.20
Recognize
In our practice, the general principle is to understand the significance of a dissection when it occurs, and this is determined by a combination of angiographic characteristics, symptoms and signs of ischaemia. Angiographic characteristics include angiographic patterns or appearances, TIMI flow, luminal compromise and clearance or persistence of contrast hang-up. Ischaemic parameters include electrocardiogram (ECG) changes, chest pain and haemodynamic compromise. It is not uncommon for spasm or recoil to occur during dissection; thus, it is imperative to obtain adequate images after the administration of intracoronary vasodilators. Table 1 shows all of the characteristics of two categories of dissection: safe to leave (type 1) and need to stent (type 2). Any individual adverse markers should prompt attention.
Table 1: Characteristics of safe-to-leave and need-to-stent categories of coronary dissection during drug-coated balloon angioplasty
| Parameters | ‘Safe-to-leave’ category type 1/non-VTD | ‘Need-to-stent’ category type 2/VTD |
| Angiography Appearance or patterns | Intraluminal filling defect, linear luminal density or haziness or extraluminal staining of contrast with rapid clearance | Long intramural contrast channels or large radiolucent spiral tracts or persistence of contrast hang-up with delayed clearance or delayed flow and abrupt closure |
| TIMI flow | 3 | ≤2
|
| Progressive luminal compromise | Absent | Present if there is encroaching/extending haematoma and in abrupt closure |
| Ischaemia (particularly persistent/progressive) | ||
| ECG changes | Absent | Present |
| Symptoms* | Absent | Present |
| Signs† | Absent | Present |
The occurrence of any characteristics within the ‘need-to-stent’ category should prompt careful evaluation.
*Symptoms include chest tightness, shortness of breath and chest pain.
†Signs include hypotension and brady or tachyarrhythmia.
ECG = electrocardiogram; non-VTD = non-vessel-threatening dissection; TIMI = thrombolysis in myocardial infarction; VTD = vessel-threatening dissection.
Management
This section provides a comprehensive explanation of each category and the modification techniques used in our DCB angioplasty practice. Concise videos of case presentations are presented in a self-explanatory manner, detailing the procedural steps, including lesion preparation algorithms, dissections and their classification based on the criteria described in Table 1. Additionally, our modification techniques, follow-up angiograms and intracoronary imaging procedures for selected cases are included. Sequent® Please NEO (B. Braun, Melsungen, Germany) paclitaxel-coated balloons are used in the video illustrations. The videos can be paused at any frame to rewind or replay if necessary. Additionally, PowerPoint presentations of each video are available for download in the supplementary material section.
Safe-to-leave category: Non-vessel-threatening dissection/type 1
We define the ‘safe-to-leave’ category as non-vessel-threatening dissection with adequate TIMI 3 flow, rapid clearance of contrast hang-up from the false lumen and absence of ischaemic signs that can be safely left without a stent as shown in Videos 1 and 2. This category typically encompasses types A, B and non-flow-limiting type C of coronary dissection, as classified by the NHLBI. A similar approach is adopted by other DCB operators. Colombo et al.7 demonstrated a target lesion failure (TLF) rate of 2.7% in lesions with untreated dissections as compared to 4.2% in lesions with no angiographic dissection (p=0.324) at a 2-year follow-up. In this study, dissections with impaired flow, significant coronary narrowing due to dissection or persistent contrast hang-up in the false lumen, defined as contrast staining for 30 s after the injection, were stented. In a study by Shin et al., there was no significant difference in TVF at a median follow-up of 3.4 years between the no angiographic dissection group and the angiographic dissection group.4 Their practice is to defer stenting types of A to C coronary dissections with TIMI 3 flow, in the absence of symptoms, ECG changes and haemodynamic disturbance. Stenting was performed for type D or higher coronary dissections and/or impaired TIMI flow. These studies reinforce the concept of good or therapeutic dissection as part of the percutaneous coronary intervention (PCI) procedure. The dissection type deemed ‘safe to leave’ based on our proposed criteria does not exhibit significantly higher cardiovascular events, as observed in the aforementioned studies.
Examples of safe-to-leave dissections
Video 1: Safe-to-leave category. (Video 1) This is a 77-year-old male with a history of limiting angina, type 2 diabetes mellitus (T2DM) managed with oral hypoglycaemic agents, paroxysmal atrial fibrillation treated with apixaban and a past smoking history, who underwent an elective angioplasty procedure. Coronary angiography showed severe stenosis in the proximal and mid left circumflex artery (LCx). The lesion in the proximal vessel was initially dilated with 2.5 × 15 mm NCB at 6 atm. The subsequent angiogram after intracoronary nitrates showed a non-VTD with quick clearance of contrast. The lesion was further dilated with an adequately sized 3.5 × 13 mm non-slip elements (NSE) Alpha™ scoring balloon at 6 atm, maintaining a safe dissection with good TIMI 3 flow. The lesion in the mid vessel was also dilated with the same balloon at 6 atm. Given that the lesions were optimally prepared for DCB, a long 3.5 × 40 mm DCB was inflated at 6 atm for 30 seconds, covering both lesions. Final angiograms in two orthogonal views showed a safe-to-leave dissection with TIMI 3 flow, rapid contrast clearance and absence of ECG changes or chest pain. Five months after the procedure, he underwent staged PCI to the left anterior descending artery (LAD) and the LCx dissection was well healed at follow–up.
Video 1: Safe-to-leave category
Video 2: Safe-to-leave category. This video demonstrates a safe-to-leave dissection during DCB angioplasty in a 58-year-old male with a background of hypertension (HTN) admitted with crescendo angina and anterior biphasic T-wave inversion. Coronary angiography showed a severe lesion after the first septal branch in a tortuous LAD. The lesion was dilated initially with smaller size 3.0 × 20 mm NCB at 8 atm, and subsequent angiography after intracoronary nitrates showed a dissection with a double lumen of contrast that cleared rapidly. Further dilatation was performed by slowly inflating a 4.0 × 13 mm NSE Alpha balloon to 10 atm, achieving full expansion and optimal lesion preparation. A 4.0 × 25 mm DCB was inflated for 30 seconds at 6 atm. The dissection remained stable throughout the procedure with TIMI 3 flow, no contrast hang-up and absence of ECG changes or chest pain; hence, it is a safe-to-leave dissection. Two years later, he was admitted with troponin-negative chest pain, and his subsequent angiogram showed well–healed dissection and excellent late lumen enlargement of the LAD with no restenosis.(Video 2)
Video 2: Safe-to-leave category
Need-to-stent category: Vessel-threatening dissection/type 2
This category defines a complex dissection where stenting or further modification is mandatory. It is characterized by impaired TIMI flow, persistent extraluminal contrast hang-up, progressive haematoma causing luminal compromise, spiral dissection and ischaemic ECG changes, symptoms or haemodynamic compromise. Prompt recognition and adopting BOS when modification has failed is crucial to restore adequate distal perfusion and resolve myocardial ischaemia.7
Examples
Video 3: Need-to-stent category. This video demonstrates a need-to-stent aorto-ostial dissection during an elective angioplasty in a 52-year-old female patient. The patient has a history of HTN, T2DM and hypercholesterolaemia. Coronary angiography showed severe ostial and mid RCA lesion, and the initial strategy was DCB angioplasty. The mid RCA was dilated with 2.5 × 15 mm NCB followed by multiple inflations of a 3.5 × 15 mm NCB until full expansion of the balloon was achieved. The ostial lesion was sequentially dilated with 2.5 × 15 mm NCB, 3.5 × 15 mm NCB and 3.5 × 13 mm NSE Alpha balloon up to 14 atm to achieve full balloon expansion. An aorto-ostial dissection was seen with persistent contrast hang-up causing progressive luminal compromise. Given the potential of extending the dissection even further into the aorta, modification was not attempted. The vessel was then subsequently stented with a 3.5 × 48 mm Synergy DES, covering both ostial and mid lesion. Intravascular ultrasound (IVUS) images post–DES showed a well-apposed stent and a well-sealed dissection. A CT aorta was performed post–procedure, which did not show any mural haematoma or aortic dissection. (Video 3)
Video 3: Need-to-stent category
Video 4: Need-to-stent category: a collection. This video shows a few examples of our need-to-stent dissections. (Video 4)
Video 4: Need-to-stent category: a collection
Modification techniques
This section covers our modification techniques to stabilize dissections. Classifying dissections by the parameters presented in Table 1 is relatively straightforward. However, there may be instances where a dissection falls into an indeterminate category, characterized by a combination of dissection, haematoma, thrombus, recoil or spasm. Occasionally, coronary spasm or no-reflow may mimic flow limitation due to luminal compromise and necessitate a comprehensive angiographic assessment after adequate administration of intracoronary vasodilator. In the setting of heavy thrombus burden, particularly in ACS, we prefer to defer any lesion preparation and DCB intervention whenever feasible. Instead, we opt for staged PCI,16,21,22 as demonstrated in the Video 7 case presentation. If thrombus aspiration and bolus administration of GPIIb/IIIa inhibitor have significantly reduced the thrombus burden and there is less no-reflow, DCB seems to be a safe strategy based on our own experience in ST-elevation myocardial infarction.16,21,22
For flow-limiting dissections, immediate repeated gentle slow low-pressure inflations, either alone or in conjunction with prolonged inflation, may stabilize dissection flaps and restore blood flow. These techniques were developed during the POBA era and demonstrated high success rates in a few studies.23–25 In 1992, Lincoff et al. analysed 109 patients with abrupt vessel closure and found that successful reversal was associated with prolonged balloon inflations (>120 seconds) (odds ratio = 6.87, p<0.001).24 Feyer et al., in 1991, followed similar techniques and also described using an oversized balloon (0.5 mm larger than the reference size) in cases of unsuccessful outcomes with prolonged inflation of a normal-sized balloon.25 This latter concept may be similar to the scoring approach we now advocate by way of extending a dissection and effectively fenestrating the false lumen.
A dissection can also be modified in the following scenarios if the patient is tolerating well:
-
Persistent extra- or intraluminal contrast accumulation with adequate distal perfusion.
-
Antegrade or retrograde extension of contrast accumulation extraluminally and within the dissection plane, indicating haematoma progression.
The theory behind this modification technique is fenestration, as described below.
Fenestration technique
Fenestration is a technique of back-bleeding a haematoma by creating a hole or tears in the dissection flap to relieve luminal obstruction.26 There are several case reports on using cutting balloons for effectively treating spontaneous, iatrogenic and stent-edge related intramural haematomas (IMHs).27–29 Scoring and NCBs have also been reported to be useful in PCI-related IMH.30 A cuttering (cutting-dottering balloon) technique was developed by Gasparini et al. to drain the haematoma by moving an inflated cutting balloon back and forth, creating tears between the false and true lumen.31
Our technique
In the event of persistent contrast hang-up indicating the development or extension of a haematoma, we use either low-pressure or prolonged or repeated inflations of a scoring balloon inflation technique, as demonstrated in Video 5. The inflations are directed towards the area of contrast hang-up and across the presumed dissection origin to fenestrate the false lumen, facilitating the drainage of IMH, as seen by clearance of angiographic contrast in Figure 1. If it is a linear, non-extensive dissection with contrast hold–up, we start with low-pressure inflations. If this fails or the dissection is deep and extensive with progressive IMH, we apply high-pressure or prolonged inflations of scoring balloons to successfully fenestrate the false lumen. Prolonged inflation may also be effective for significant recoil. In instances where the scoring balloon fails, a cutting balloon downsized by 0.5 mm diameter can be inflated at low pressures to facilitate this process. Occasionally, the haematoma may extend beyond the target lesion, necessitating focused balloon inflations on such segments to achieve successful resolution, as illustrated in Video 6. It is crucial to conduct angiographic assessment after administering an adequate bolus of intracoronary vasodilators following the inflations. In the event of repeated failed attempts to modify dissections into a safe category, BOS should be performed, as demonstrated in Video 7.
Figure 1: Illustration of fenestration technique
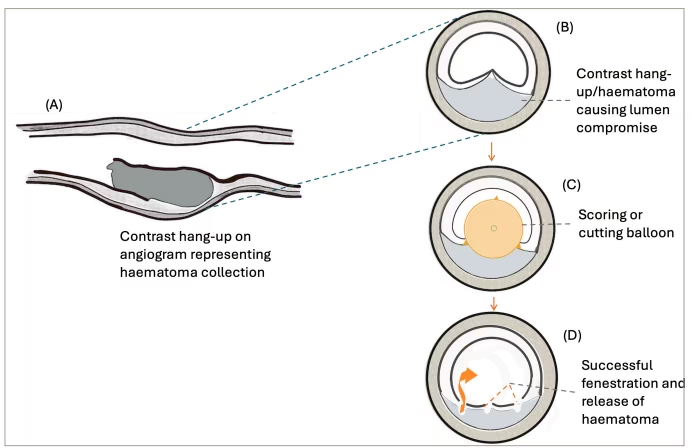
A represents an intimal-medial flap with contrast hang-up in the dissection plane, resulting in luminal compromise; B presents the cross-sectional view of the contrast hang-up segment; C illustrates the scoring or cutting elements of an inflated balloon at the location of contrast hang-up; D demonstrates a successful fenestration technique; tears or holes are created, effectively draining the haematoma and facilitating rapid contrast clearance on angiography
In our practice, the choice between prolonged balloon inflation with a cutting or scoring balloon for dissection modification is guided by lesion behaviour, cost and availability. When there is contrast hold-up or a dissection flap, we consider fenestration with either scoring or cutting balloons. Cutting balloons are preferred when a more controlled or deeper modification is required, especially in resistant lesions, whereas scoring balloons are used when a gentler approach is suitable. In addition to clinical factors, cost and availability also influence decision-making. Scoring and cutting balloons can be resource-intensive and not always readily available in all centres, which sometimes necessitates adapting the strategy based on practicality as well as lesion characteristics.
Video 5: Modification of dissection into a safe category by repeated balloon dilatations. This video demonstrates the modification of a mid-RCA dissection with persistent contrast hang-up into a safe category using repeated balloon dilatation with NSE Alpha balloon. A 59-year-old female with significant triple-vessel coronary disease who declined coronary artery bypass grafts (CABG) due to complex comorbidities, including two cerebrovascular accidents, bipolar disorder, ACS and myalgic encephalomyelitis. She had previous DCB to the LAD, first diagonal and second obtuse marginal branch. She was admitted for an elective angioplasty to a severe stenotic lesion in the mid RCA. The lesion preparation was performed with low-pressure inflations of a 3.0 × 15 mm NCB at 6 atm, followed by treatment with a 3.0 × 20 mm DCB at 6 atm. Post-DCB angiogram after intracoronary nitrates revealed a dissection with persistence of extraluminal contrast retention in two orthogonal views and TIMI 3 flow with no ECG changes. Given the persistence of contrast hang-up, the dissection was modified by inflating a 3.0 × 13 mm NSE Alpha balloon at the site of contrast hold–up. Subsequently, there was a rapid clearance of contrast, thereby achieving successful modification into a safe category with rapid contrast clearance. During her recent clinical follow-up after 4 years, she has remained asymptomatic with no occurrence of TLF. (Video 5)
Video 5: Modification of dissection into a safe category by repeated balloon dilatations
Video 6: Modification of dissection into safe category by prolonged high inflations. This video illustrates the technique of prolonged high-pressure inflation technique for 30–60 seconds, as part of our routine DCB practice, to modify an extensive dissection into a safe category with no contrast hang-up at the end of the procedure. The patient was 57 years old with a history of T2DM and hypercholesterolaemia. Coronary angiogram showed severe stenosis in the mid LCx and obtuse marginal one (OM1) was a small calibre vessel with mild ostial disease. The strategy was to treat the mid LCx lesion while preserving the small OM1. The lesion was prepared adequately with a 2.5 × 20 mm NCB, a 3.5 × 20 mm NCB at 6 atm followed by a 3.5 × 13 mm NSE Alpha balloon at 14 atm. Subsequent angiography revealed a dissection extending throughout the lesion and persistent extraluminal contrast with TIMI 3 flow at the proximal segment. In the distal segment, there was some luminal compromise indicating extension of dissection and haematoma. Through repeated prolonged inflation of a 3.5 × 13 mm NSE Alpha balloon from the proximal to distal lesion, the dissection was successfully fenestrated, rapidly clearing the contrast. No contrast hang-up was observed post-modification. The lesion was subsequently treated with 3.5 × 40 mm DCB. During his staged pressure-wire assessment of the LAD after 6 weeks, the treated segment of LCx exhibited good lumen gain and a healed dissection. (Video 6)
Video 6: Modification of dissection into safe category by prolonged high inflations
Video 7: Need-to-stent category after failed modification attempts. A 41-year-old male with T2DM was admitted with chest pain and lateral ST elevation. The index angiogram revealed thrombotic distal left main stem (dLMS) and proximal LAD (pLAD) lesion. He received 48 hours of tirofiban to stabilize the thrombotic lesion and subsequently returned to the catheterization laboratory for further optical coherence tomography (OCT) assessment after a multi-disciplinary team meeting. OCT revealed plaque rupture with red thrombus and severe fibrous disease extending from the distal LMS to the proximal LAD. Given his young age and diabetes, we initially opted for a DCB approach. The dLMS lesion was dilated with a 3.0 × 20 mm NCB, a 4.0 × 12 mm NCB followed by treatment with a 4 × 15 mm DCB, whereas the pLAD lesion was prepared with a 3.0 × 15 mm NCB followed by a 3 × 20 mm Scoreflex and treated with 3 × 30 mm DCB. However, following DCB treatment, persistent contrast retention was observed on angiography, and OCT demonstrated an intimal-medial flap with a haematoma at the proximal end of the flap adjacent to the ostium of the LAD. There was excellent acute lumen gain in the LMS after DCB. A 3 × 20 mm Scoreflex was inflated at the proximal contrast hang-up part of the dissection at 6 atm, followed by a larger-size 3.5 × 13 mm NSE Alpha balloon at low pressure of 4 atm. Subsequent attempts at modification failed, and the dissection flap in the LAD was sealed by deploying a stent as visualized on OCT. The accompanying video provides a detailed demonstration of the modification techniques used. (Video 7)
Video 7: Need-to-stent category after failed modification attempts
In many of our presented cases, the NCB was inflated at 6 atm. During lesion preparation, our practice is to initially inflate the NCB to low pressure at 6 atm. If full balloon expansion is achieved at this stage, we interpret this as an indication that the lesion is adequately dilated. In such cases, further increasing the inflation pressure is unlikely to provide additional benefit and may instead increase the risk of vessel trauma. Our approach prioritizes minimizing vessel injury while simultaneously ensuring effective lesion preparation and cost-effectiveness. In most cases, we opt for NCB balloons as the initial dilatation balloon due to their cost-effectiveness compared to scoring or cutting balloons. Lesion preparation with NCB alone may be optimal.
The decision to modify an indeterminant category to a safe category increases with experience, and discussions with other colleagues during the procedure could also be helpful. BOS is a safe option when faced with dilemmas in such scenarios, particularly during the initial stages of DCB angioplasty.
Conclusion
This article presents our experiences and practice of dissection management in the setting of DCB angioplasty, developed over the last decade at Norfolk and Norwich University Hospital. While DCB angioplasty presents a learning curve, coronary dissection remains a significant barrier to its widespread adoption. By adopting the ARM strategy to categorize dissections into two simple categories based on distal perfusion, symptoms and signs of ischaemia, and establishing a reasonable threshold for BOS, the learning curve may be safely shortened.











