Despite advancements in mortality rates from cardiovascular disease (CVD) over the last 50 years, it remains the leading cause of death for women and the third leading cause for women aged 18 to 44.1 A 2011 report from the American Heart Association (AHA) starkly states that one in every two women will die from a cardiovascular-related disorder.2 With the increasing prevalence of metabolic syndrome and obesity, the urgency of focusing on the early identification of dyslipidaemia to enhance the primary prevention of CVD cannot be overstated.
Women have been found to have an increasing prevalence and incidence of dyslipidaemia, with an estimated 40.4% of women having a total cholesterol (TC) level >200 mg/dL.3 Dyslipidaemia and the development of atherosclerotic cardiovascular disease (ASCVD) in women are associated with the highest population-attributable risk for myocardial infarction (MI) when compared to other CVD risk factors such as smoking, diabetes or obesity.4 However, although >90% of women have at least one CVD risk factor defined by the AHA and the United States Preventive Services Task Force (USPSTF), as many as 50% of this population are not screened appropriately with surveillance lipid panels.5 Even when women are screened, the female sex is associated with a lower likelihood of receiving statin therapy compared to the male sex, suggesting that many women with dyslipidaemia are not being diagnosed and treated appropriately.6 Women are less likely to be prescribed high-intensity statin therapy and achieve low-density lipoprotein cholesterol (LDL-C) goals, despite having risk factors. They are also less likely to receive non-statin lipid-modifying medications.7,8 The potential consequences of these disparities are severe, including increased mortality rates and reduced quality of life. In this article, we highlight disparities in the screening, diagnosis and treatment of women with dyslipidaemia. We also provide a call to action to continue evidence-based treatment of dyslipidaemia and focus on strategies to advance women’s cardiovascular health.
A brief overview of the physiology of lifetime lipids in women
Female physiology causes more significant fluctuations of lipid levels throughout the lifespan. Before adolescence and early adulthood, lipid levels are generally similar between men and women, except for fluctuations associated with the menstrual cycle and pregnancy, which can cause an increase in lipid levels of up to 50%.9 Men generally have a shorter time to peak cholesterol development (45–49 years), while women reach peak cholesterol about 10 years later in their mid-50s.10
In adolescence, paediatricians perform universal screening lipid panels on children who are thought to be at risk for metabolic syndrome. These panels are usually obtained when the children are 9–11 years old and 17–21 years old to identify higher-risk individuals, including those with genetic disorders such as familial hyperlipidaemia.11,12 If a child is found to have high lipid levels, the first recommendation is lifestyle modification, followed by statin therapy. As mentioned above, fluctuations in lipid levels are associated with the menstrual cycle; therefore, clinicians must consider this when screening adolescent females for lipid disorders. Normal lipid panel variation is estimated at 5–8%. TC and LDL-C levels rapidly increase after menses and peak in the follicular phase before declining throughout the luteal phase. However, meta-analysis of triglyceride (TG) levels during the menstrual cycle has found that levels do not fluctuate a clinically significant amount. The rise and peak of TC and LDL-C correspond to the oestrogen peak during the menstrual cycle, whereas the decline corresponds to the progesterone peak.13
Many teenage girls will initiate contraception during the years they are being screened for dyslipidaemia. The National Lipid Association (NLA), a leading authority in lipid management, has found that specific birth control methods, such as oral contraceptive pills (OCPs), can cause an increase in TG levels, particularly those formulations of OCPs that have higher concentrations of oestrogen.14 There are currently no guidelines on when to screen women during the menstrual cycle, but a suggestion is to compare like samples. Of note, as metabolic syndrome increases in this young population, a higher proportion of women have been diagnosed with polycystic ovarian syndrome (PCOS), affecting an estimated 5–13% of the population.15 This syndrome is characterized by menstrual irregularity or amenorrhoea, hyperandrogenism, insulin resistance and polycystic ovaries. PCOS can be associated with dyslipidaemia and increased CVD risk; these patients should be counselled on lifestyle management and have aggressive screening for dyslipidaemia, with international guidelines recommending every 6–12 months.16–18
Transitioning from adolescence into adulthood, new factors influence lipid levels in women, particularly pregnancy. Several studies have found that unfavourable CVD risk factors in the pre-pregnancy period, including dyslipidaemia, are associated with an increased risk of developing pregnancy complications such as pre-eclampsia.19 An analysis of patients in the Framingham Heart Study analysed over 500 parent–offspring pairs after measuring LDL-C before the offspring’s birth. It concluded that high maternal pre-pregnancy LDL-C levels are associated with high adult offspring LDL-C levels, even when accounting for lifestyle, anthropometric and inherited factors, suggesting possible epigenetic changes.20 In an analysis of data from the National Health and Nutrition Examination Surveys from 1999 to 2014 of women aged 20–44, only 39% of pregnant women had ideal cholesterol levels, suggesting that pre-pregnancy diagnosis and treatment of dyslipidaemia may miss many women who would benefit from it.21
Women experience increases in TC and TGs during pregnancy, peaking at term delivery. TC is estimated to increase between 35 and 37% in uncomplicated pregnancies. TGs increase between two– and three–times baseline levels.22 Higher levels of TC, TG, LDL-C and lower high-density lipoprotein cholesterol (HDL-C) have been associated with adverse outcomes, such as preterm birth, gestational diabetes and pulmonary embolism.23 There are no screening guidelines for dyslipidaemia in pregnant women. Screening before pregnancy is considered the most beneficial, which is the current recommendation of the NLA.24 If abnormal values are found, they should be monitored during pregnancy and followed up at 6 weeks postpartum.21 In a Journal of the American College of Cardiology (JACC) update on recommendations for primary prevention in women, it is recommended that women experiencing adverse pregnancy outcomes (APOs) such as gestational hypertension (HTN), gestational diabetes, intrauterine growth restriction, placental abruption, obesity, sleep disorders and maternal age >40 years undergo cardiovascular screening within 3 months of postpartum.18
Until recently, there were limited effective options to treat dyslipidaemia during pregnancy due to the contraindication label of statins by the Food and Drug Administration (FDA).25 In 2021, the FDA requested the removal of that classification, and the current recommendation is that treatment decisions should be made individually, based on the patient’s risk profile, and through shared decision-making between the patient and clinician.26 According to the NLA, clinicians can consider other therapies, such as bile acid sequestrant colesevelam and LDL-C apheresis in extreme cases.27 Ezetimibe has been associated with adverse foetal effects in animal studies and is not recommended, and the safety or efficacy of PCSK9 inhibitors has not been determined in pregnancy.27 In rare cases, such as gestational hypertriglyceridaemia-induced pancreatitis, it might be necessary to perform therapeutic plasma exchange, as there is significant morbidity and mortality associated with this condition.28
After menopause, when women lose the mediating effects of oestrogen, their overall lipid levels tend to be higher compared to men, increasing their risk of CVD during the latter half of life.29 Menopause is associated with an atherogenic lipid profile with increased LDL-C and TC and a decline in HDL-C levels. In one meta-analysis, women experienced an annual increase of 1.5 mg/dL and 1.2 mg/dL in TC and LDL-C levels, respectively, following menopause.30 Certain factors have been linked to early menopause, such as smoking, autoimmune disease, low socioeconomic status and Black or Hispanic race, suggesting that these groups should have more aggressive screening for dyslipidaemia, given that they are at increased risk for cardiovascular morbidity and mortality.31,32 Menopause has also been associated with an increase in waist circumference, increased central adiposity, loss of skeletal muscle and an increase in fat mass due to oestrogen deficiency, which in turn increases CVD risk.33 The factors influencing cholesterol in women across their lifespans are illustrated in Figure 1.21,34
Figure 1: Physiology of lipids across the female lifespan and factors influencing lipid levels21,34
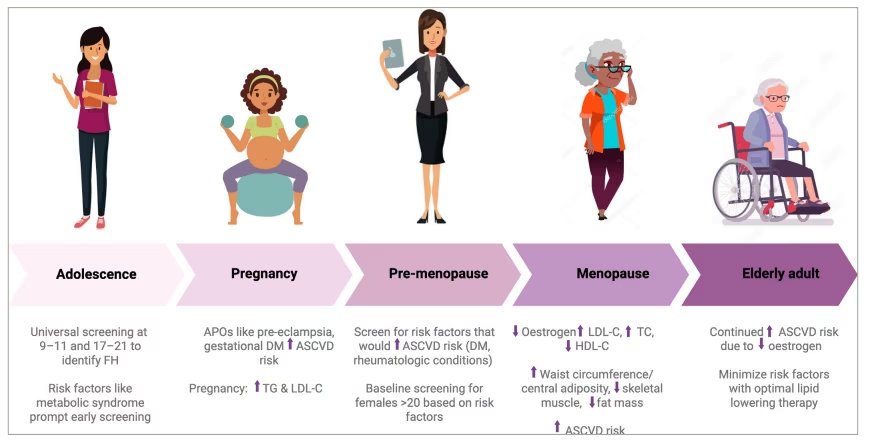
FH = familial hyperlipidaemia; APOs = adverse pregnancy outcomes; ASCVD = atherosclerotic cardiovascular disease; DM = diabetes; HDL-C = high-density lipoprotein cholesterol; LDL-C = low-density lipoprotein cholesterol; TC = total cholesterol; TG = triglyceride.
Factors influencing dyslipidaemia change throughout a woman’s life, illustrating how crucial proactive screening is for reducing future CVD risk. However, as discussed in the next section, younger women rarely undergo screening, even with increasing risk factors in this population, such as obesity, insulin resistance and metabolic syndrome. It is the authors opinion that most women are currently being under-screened for dyslipidaemia.
Sex disparities in screening
The AHA and USPSTF publish recommendations for screening for dyslipidaemia, which are outlined in the following paragraph. However, many of these guidelines recommend different ages for initial screening based on the presence or absence of CVD risk factors, creating confusion. The AHA recommends screening adults older than 20 who are not on lipid-lowering therapy to document their baseline ASCVD risk and LDL-C levels.34 The USPSTF updated its guidelines in 2022 to recommend screening all adults aged 40–75 with one or more cardiovascular risk factors and treating them with a statin if a 10-year CVD risk is 10% or greater based on pooled cohort equations (PCEs).35 Before these updated guidelines, the USPSTF recommended screening men at 35 years old and women at 45 for dyslipidaemia.36
The presence of CVD risk factors should prompt earlier screening by health professionals for women and men alike. These factors have been modelled in PCEs, such as the 10-year ASCVD risk calculator, which takes into account a patient’s age, sex, race, systolic and diastolic blood pressure, cholesterol panel, presence of diabetes, smoking history and previous treatment for HTN or dyslipidaemia, or aspirin therapy to estimate the 10-year risk of ASCVD events.37 The presence of more CVD risk-enhancing factors should prompt earlier screening of patients. The AHA defines these risk factors as a family history of premature ASCVD (males<55 and females<65), primary hypercholesterolaemia, metabolic syndrome, chronic kidney disease, inflammatory conditions such as rheumatoid arthritis, lupus or HIV/AIDS, a history of premature menopause (before age 40 years) and a history of APOs that increase lifetime ASCVD risks. Other risk factors such as pre-eclampsia, high-risk race or ethnicity (South Asian ancestry), persistently elevated lipids or biomarkers such as TGs, high-sensitivity C-reactive protein or lipoprotein(a) and/or apolipoprotein B can also increase ASCVD risk and should be accounted for.38,39 The USPSTF denotes similar risk factors that should prompt earlier screening, such as a history of diabetes, HTN, smoking, obesity and a family history of CVD.40 The current screening recommendations from the AHA and USPSTF are outlined in Figure 2.31,32
Figure 2: A comparison of current AHA/ACC and USPSTF recommendations for lipid screening31,32
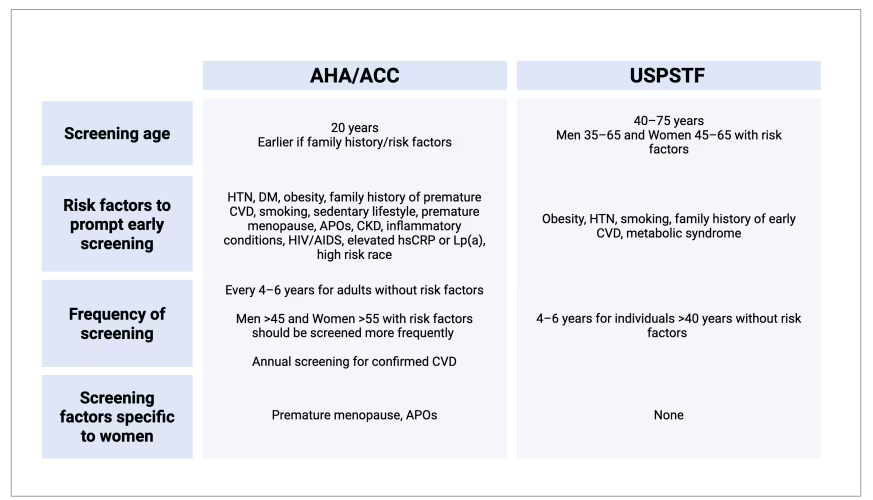
ACC = American College of Cardiology; AHA = American Heart Association; APOs = adverse pregnancy outcomes; CVD = cardiovascular disease; DM = diabetes; HTN = hypertension; USPSTF = United States Preventive Services Task Force; CKD = chronic kidney disease; hsCRP = high-sensitivity C-reactive protein; Lp(a) = lipoprotein (a)
In a study of adults in the USA using National Health and Nutrition Examination Survey data, 55% of women aged 20–44 and 74.2% of women older than 45 were considered USPSTF-at-risk with one or more CVD risk factors. Nearly all reproductive age and older women were AHA-at–risk (99.5 and 99.6%). In the same sample, 96.8% of women had seen a healthcare professional within the previous 3 years, but only 62.1% reported having a cholesterol test in the past 5 years.5 This suggests that while women maintain their recommended annual health maintenance, they are not appropriately screened for dyslipidaemia. Many clinicians use risk calculators to estimate the 10-year risk of ASCVD, and newer iterations of these calculators, notably the AHA PREVENT calculator, factor in kidney disease and even geographic location as predictors of future CVD events.41 However, there is not currently a calculator that considers peripartum complications such as pre-eclampsia or gestational HTN that have been associated with increased lifetime risk; many women’s risk is likely undervalued.39
The ACC estimates that eight out of every ten women of childbearing age have never had a lipid assessment.42 Earlier screening for dyslipidaemias could be part of perinatal care. This would vastly increase the number of women who are screened. There have also been reports of a correlation between dyslipidaemia, preterm birth and low gestational weight with lifetime risk for CVD. In one study of 1,112 women who were screened at a postpartum visit for dyslipidaemia, 7% had elevated TC, and 13% had elevated TGs. The sample contained 5,101 women, and factors that were associated with screening were race (White), older age and having a diagnosis of coronary artery disease (CAD), HTN and diabetes.43 Identifying dyslipidaemias early in life helps patients and physicians focus on risk modification and early initiation of pharmacotherapy to reduce clinically significant CVD.
Sex disparities in diagnosis and treatment
An estimated 15.5 million Americans over the age of 20 have CVD, and the prevalence increases every year, with a projected 18% increase by 2030.44 The 2018 AHA/ACC cholesterol guidelines define dyslipidaemias as high TC (TC>240 mg/dL), high LDL-C (LDL-C>100 mg/dL) and/or high TGs (TG>150 mg/dL).34 Early identification and treatment are the hallmarks of primary and secondary prevention of CVD.34,45 The current recommendation is to use a combination of a healthy diet and exercise with high-intensity or maximally tolerated statin therapy to reduce LDL-C by at least 50% in patients with clinical CVD. Statins are the primary recommended pharmacologic treatment in patients who have clinically evident ASCVD, severe hypercholesterolaemia with an LDL-C>190 mg/dL, and diabetes in adults aged 40–75 years.34 A fourth group where statin therapy is recommended is primary prevention in groups that PCEs estimate as being high risk (≥20%), intermediate risk (≥7.5% to <20%) or borderline risk (5% to <7.5%) based on risk enhancers, presence of elevated coronary artery calcium score and clinician–patient discussion.18 The ACC outlined these recommendations in 2019, which are summarized in Figure 3.18,38 There are no differences in recommendations based on biological sex in the current ACC/AHA guidelines.
Figure 3: ACC recommendations from 2019 for the initiation of statin medication in women18,38
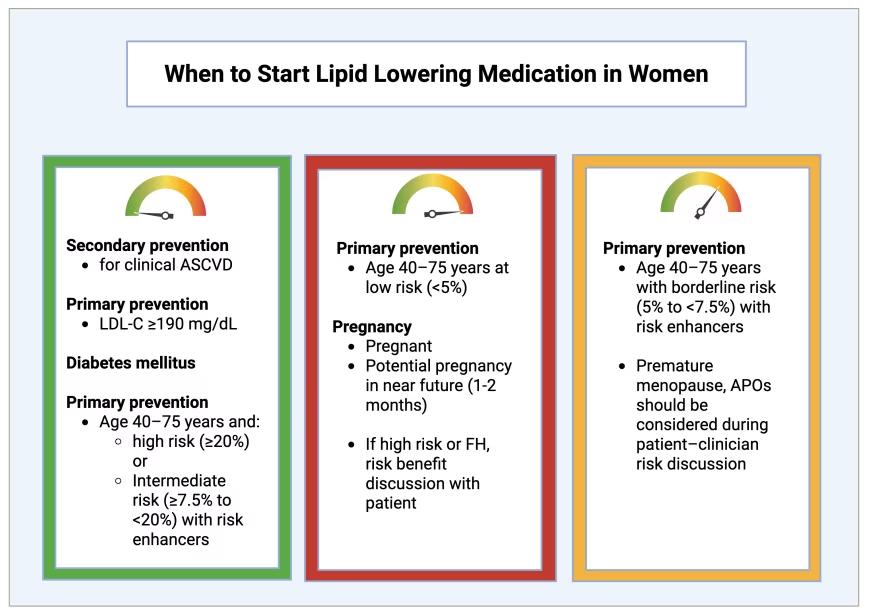
Green box: Statin therapy generally indicated. Red box: statin generally not recommended. Yellow box: statin may be considered.
Risk enhancers include APOs and premature menopause; clinicians should remember to take a comprehensive obstetrical history and discuss any potential risk factors that would indicate the need for statins for primary prevention.
APOs = adverse pregnancy outcomes; ASCVD = atherosclerotic cardiovascular disease; LDL-C = low-density lipoprotein cholesterol; FH = familial hyperlipidaemia
In a sample of nearly 60,000 age- and sex-matched Spanish patients included in the ESCARVAL-GENERO study, 18% met the diagnostic criteria for dyslipidaemia but did not have an associated diagnosis or receive prescribed treatment. Female sex was significantly associated with this diagnostic inertia, with the proportion of women fitting this description being higher than that of men (20.1% compared to 15.8%).46 In a similar study of the Patient and Provider Assessment of Lipid Management (PALM) registry, 5,693 adults were recommended for statin therapy, with 26.5% not on treatment. Of those patients, 59.2% reported never being offered a statin. Those patients were more likely to be female (odds ratio [OR], 1.22), Black adults (OR, 1.48) and those without insurance (OR, 1.38).47 Factors that have been shown in other studies to be positively associated with screening are women who are White with a prior history of CAD, HTN or diabetes.48,49 In a sample of 600,000 patients containing 41.7% women in the USA with established risk factors for CVD, 49.9% were not on any statin therapy, and those patients were more likely to be female with higher comorbidities.50 Additional studies have been completed comparing statin prescriptions for Black and White women, with Black women having much lower odds of being prescribed statin therapy.51
Lifestyle modification and aerobic exercise are the initial recommendations listed in many CVD guidelines for dyslipidaemia.52 This is supported by the INTERHEART study, which assessed modifiable risk factors such as smoking cessation, vegetable and fruit consumption, and regular physical activity, where intervention reduced the risk of MI by 80%.4 While lifestyle modification is essential, it remains unclear whether this benefit is equal between sexes, and it appears to be more beneficial to men. In the ‘Prevención con Dieta Mediterránea’ or PREDIMED trial (ISRCTN35739639), lifestyle changes, such as adopting a Mediterranean diet, were initially shown to reduce cardiovascular events (myocardial infarction, stroke or death from cardiovascular causes).53 When separating the control versus intervention group by sex, the female subgroup showed no endpoint difference compared with the control, and the publication was later retracted.54
If the first tier of recommendations has not been shown to benefit women, it would be expected to see more female patients on statin medications. The opposite is true. In many studies of prescriber behaviour and dyslipidaemia treatment, women are less likely to be prescribed a statin than men, especially younger women.50,55,56 In the GOULD observation registry of patients receiving lipid-lowering therapy, women are also less likely to be offered intensification of statin therapy or achieve an LDL <70 mg/dL goal compared to men (23.2% versus 32.4%). This is further compounded by low rates of intensification of lipid-lowering therapy for people of non-White race and Hispanic ethnicity.57
Regarding other lipid-lowering medications, women are less likely to have intensification or additional drug additions, even though, as mentioned above, they are less likely to achieve the LDL-C goal. Some drugs have been shown to have preferential benefits for women in clinical trials. For example, the IMProved Reduction of Outcomes: Vytorin Efficacy International Trial orIMPROVE-IT trial (NCT00202878), which tested ezetimibe, showed that it reduced LDL-C equally in men and women; however, it significantly lowered the incidence of adverse cardiac events by 12% in women but only by 5% in men.58,59 In another recent study of four phase III clinical trials of the drug bempedoic acid, an inhibitor of ATP citrate lyase which works upstream of HMG-CoA enzyme that is affected by statins, women were shown to be 1.6 times more likely than men to achieve a minimum LDL-C reduction of 30% in 12 weeks compared to placebo.60 While these drugs have been shown to lower LDL-C in women and are effective therapies to achieve LDL-C goals, few women are escalated to these therapies in combination with statins. Since 2018, guidance has been published by the ACC/AHA recommending non-statin medications be used in combination with statin therapy to achieve LDL-C goals.34 There are currently no diagnostic or treatment guidelines that differentiate patients based on biological sex.
Several factors have been hypothesized as reasons for the lack of recognition and treatment of CVD in women. Subpar screening of at-risk women was previously discussed and is a significant factor in the lack of primary prevention initiation. Women are also more likely to have atypical coronary syndromes and have missed or delayed MI diagnoses. This leads to a decrease in the use of statins in secondary prevention and a reduction in overall statin use and intensification.52,61 Statin therapy remains the mainstay of treatment for secondary MI prevention, even in women with MI with non-obstructive coronary arteries.52,62 Another factor is the teratogenicity of statin therapy and the hesitance to use it in women of childbearing age, although this is no longer a current recommendation of the FDA.26 These factors alone do not explain the lack of statin therapy or LDL-C goal achievement in women. The initiation of statin therapy is driven in large part by PCEs, which often underestimate CVD risk for younger patients, particularly women.52,63 Women with high LDL-C levels might have a deferral of pharmacotherapy as their estimated 10-year risk of MI or stroke is low. However, as previously mentioned, many factors that increase the risk of CVD are not accounted for in PCEs. Additionally, elevated HDL-C levels provide false reassurance in women against the development of future CVD when high LDL-C levels are present; clinicians should instead use a combination of risk factors and PCEs to guide equal and early treatment.64,65 A recent recommendation by the ACC/AHA was to use the above risk-enhancing factors with existing calculators to create a more detailed risk profile.66
When women are offered statin therapy, they are more likely to decline or distrust the medication, not believing it to be safe or effective.55 Studies of statin use in the USA also found that women are more likely to report statin-associated muscle symptoms and thus discontinue therapy.67 Another found that women were more likely to try three or more statins but less likely to be treated with alternative lipid-lowering medications. Overall, the study found women to be more dissatisfied with their statin medication and the way their provider explained the treatment, leading to non-compliance.8 This suggests that not only do women experience a higher risk of side effects from statins, but there is also a lack of sufficient counselling from providers about the importance of statin therapy. Clinicians must be comfortable with counselling on future CVD risks and use shared decision-making with patients to increase buy-in for treatment.
Future lens: Areas of improvement
In previous sections, we have highlighted several strategies to increase the screening, diagnosis and treatment of women with dyslipidaemia. Still, as more therapies for reducing cholesterol are developed, evaluating treatment groups for these research trials is essential. In several landmark trials, including REDUCE-IT (Evaluation of the Effect of AMR101 on Cardiovascular Health and Mortality in Hypertriglyceridemic Patients With Cardiovascular Disease or at High Risk for Cardiovascular Disease: REDUCE-IT [Reduction of Cardiovascular Events With EPA – Intervention Trial]; ClinicalTrials.gov identifier: NCT01492361), FOURIER (A Double-blind, Randomized, Placebo-controlled, Multicenter Study Assessing the Impact of Additional LDL-Cholesterol Reduction on Major Cardiovascular Events When Evolocumab [AMG 145] is Used in Combination With Statin Therapy In Patients With Clinically Evident Cardiovascular Disease; ClinicalTrials.gov identifier: NCT01764633) and IMPROVE-IT (A Multicenter, Double-Blind, Randomized Study to Establish the Clinical Benefit and Safety of Vytorin [Ezetimibe/Simvastatin Tablet] vs Simvastatin Monotherapy in High-Risk Subjects Presenting With Acute Coronary Syndrome [IMProved Reduction of Outcomes: Vytorin Efficacy International Trial – IMPROVE IT]; ClinicalTrials.gov identifier: NCT00202878), which significantly impacted guideline-directed medical therapy for dyslipidaemia, the proportion of women in these trials was less than 30% (29, 25 and 24%, respectively).59,68–72 In trials from 1990 to 2018 involving lipid-lowering agents and overall enrolment of women, the average participation rate is only 29%.73 That number drops even further when looking at the inclusion of minority groups; one meta-analysis of the 35 trials of cardiometabolic drugs over the previous 10 years found that only 4% of participants were Black, 12% Asian and 11% Hispanic, with no increasing trends observed.74 This suggests that many lipid-lowering medications are not being tested on a large number of diverse women, and their true potential or side effects are not accounted for. Trials usually exclude women of childbearing age, but women are still underrepresented, given the prevalence of dyslipidaemia. It is paramount to test new lipid-lowering medication adequately in women so that providers can be assured of drug effectiveness.64
Additionally, few, if any, of the principal investigators on these clinical trials were women, with a recent analysis showing that only 10.1% of clinical trial committee members were women, and more than half of the trials had no women in clinical trial committee roles.75 Another study of over 100 heart failure trials conducted between 2000 and 2019 revealed that only 11% of trial leadership positions were held by women, and this number had not increased significantly over the last 20 years.76 Compared to trials led by men, women-led studies were more likely to enrol a higher proportion of female participants (37.9% compared to 44.9%). This suggests that increasing the number of female principal investigators may lead to a greater representation of female study participants and more accurate results from lipid-modifying therapies in female patients. A potential pipeline of increased female participation in clinical cardiology research is outlined in Figure 4.76
Figure 4: A potential pipeline to increase female representation in clinical trials
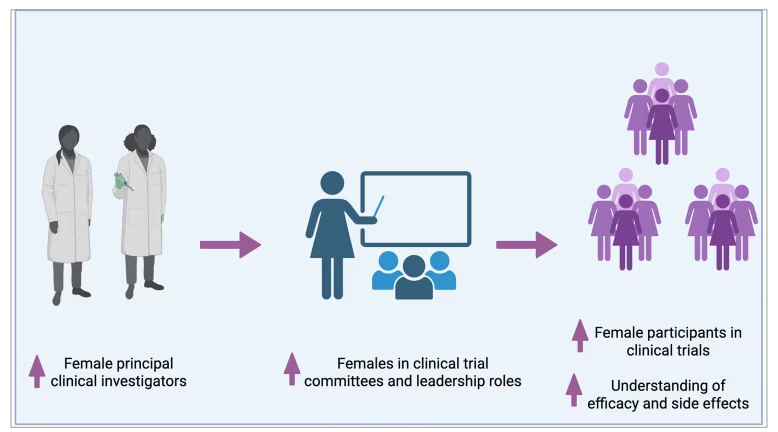
Trials with female principal investigators and in committee leadership roles recruit more female participants.76 Figure represents a potential pipeline for increasing female participants in research studies
Conclusion
As discussed, dyslipidaemia and CVD remain a significant concern for women in the 21st century, and the number of female patients with CVD is expected to increase over the next 20 years.3,64 The medical community has been historically poor at screening women, starting lipid-lowering therapy, achieving LDL-C goals and including women in clinical trials. This article aims to draw attention to an issue that remains a key concern in women’s health. Increasing awareness of the current state of screening and pharmacological therapy will ideally bring this to clinicians’ attention as we work to improve these numbers. Additionally, we hope that with this increased visibility of the disparities we have outlined above, special attention is brought to the design of clinical trials concerning sex representation and female representation in leadership roles to assess pharmacological interventions for CVD in women adequately.