
Hypertension has been associated with increased cardiovascular morbidity and mortality, as well as with overall elevated all-cause mortality.1 Prevalence increases with age, affecting 28.5% of US individuals aged 20–44 years, 58.6% of those aged 45–64 years and 76.5% of those aged 65 years and older.2 In addition to its clinical burden, hypertension poses a substantial economic challenge, representing 30% of total expenditures, which is the largest share of direct healthcare costs (including prescription medications and office-based visits).2 Resistant hypertension (rHTN) is defined as blood pressure (BP) above goal despite treatment with three antihypertensive medications with complementary mechanisms of action, including a diuretic at maximally tolerated doses, or BP at goal but requiring ≥4 medications.3 The prevalence of patients receiving treatment with rHTN in the USA is approximately 19.7%, affecting an estimated 10.3 million adults.4 Furthermore, rHTN is associated with a significantly increased risk of adverse cardiovascular outcomes, such as myocardial infarction, heart failure, stroke, chronic kidney disease (CKD) and cardiovascular mortality.2 Additionally, rHTN is more common in non-Hispanic Black/African American patients, which may be related to social factors, and can further exacerbate renal disease progression.3,5
The most current 2025 American Heart Association/American College of Cardiology (AHA/ACC) High Blood Pressure (HBP) Guideline for the Prevention, Detection, Evaluation and Management of High Blood Pressure in Adults (AHA/ACC HBP Guideline) recommends the addition of a mineralocorticoid receptor antagonist (MRA) as a fourth-line agent.3 However, its use is often limited in patients due to antiandrogenic side effects or in those with underlying kidney disease due to hyperkalaemia. When direct contraindications against MRAs as listed above are present, then other alternative drugs such as aprocitentan may be used as fourth- or fifth-line therapies.3,6 In addition, many existing therapeutic approaches fail to address alternative mechanisms contributing to rHTN. One such mechanism involves the endothelin pathway, specifically endothelin-1 (ET-1), a potent vasoconstrictor implicated in vascular dysfunction, inflammation and sodium retention.6 Until recently, this pathway has remained largely untargeted in clinical practice.
Aprocitentan, a novel, once-daily oral dual endothelin receptor antagonist (ERA), has emerged as a promising therapeutic candidate for rHTN.7 Recent clinical trial evidence has demonstrated its efficacy in lowering BP in patients unresponsive to conventional therapies, offering a new avenue in the management of this high-risk population. This article aims to explore the clinical evidence supporting the use of aprocitentan for rHTN, its mechanism of action, its potential role in clinical practice and its description in the most recent AHA/ACC HBP Guideline. In addition, we will examine its indications, contraindications and safety profile, highlighting its potential to address a significant unmet need in hypertension management.
Endothelin’s role in cardiovascular health
The endothelin system is composed of three 21-amino acid peptides and acts primarily through two G protein-coupled receptors, endothelin A (ETA) and endothelin B (ETB).7 This system is a key pathway in hypertension.7 The ETA receptors mediate vasoconstriction and vascular remodelling via calcium-dependent pathways such as Rho kinase, while ETB receptors facilitate nitric oxide and prostaglandin release, contributing to vasodilation and promoting sodium and water excretion by the kidneys.7 ET-1 production is stimulated by some factors, including hypoxia, angiotensin II, catecholamines and thrombin, and is inhibited by nitric oxide and prostaglandins.6 Moreover, angiotensin II potentiates ET-1’s vasoconstrictive effects. Notably, endothelin also influences sympathetic nervous system activity by promoting catecholamine release and modulating baroreceptor function.7
Patients with rHTN often exhibit heightened activity of the endothelin system, characterized by elevated levels of ET-1.8 Beyond its potent vasoconstrictive properties, ET-1 contributes to adverse vascular remodelling and exacerbates inflammatory process factors, which may play a critical role in the progression of hypertension and its associated complications, including heart failure and CKD.8 A dual endothelin receptor antagonism can mitigate these effects by inhibiting signalling at the ETA and ETB receptors, causing vasodilation and thereby reducing BP.8 Such a mechanism will lead to a decrease in vascular resistance by inhibiting the ETA receptor, while also preventing overstimulation of the ETB receptor, which could otherwise lead to increased aldosterone levels. Overall, this new therapeutic avenue can help address the multifactorial nature of rHTN. Figure 1 summarizes the various mechanisms of action of the currently available medications for BP, including ERA.
Figure 1: Mechanisms involved in the regulation of blood pressure and its therapeutic targets
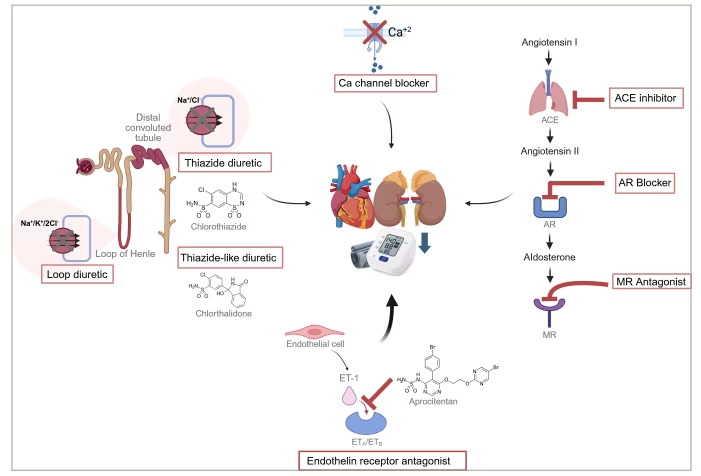
ACE = angiotensin-converting enzyme; AQ = angiotensin receptor; Ca+2 = calcium; Cl- = chloride; ETA = endothelin A; ETB = endothelin B; K+ = potassium; MR = mineralocorticoid receptor; Na+ = sodium.
Evolution of endothelin receptor antagonist therapy
The pharmacological landscape of ERAs is both diverse and evolving, shaped by differences in pharmacokinetics, receptor selectivity and safety profiles that have influenced their therapeutic applications. Originally, this drug class was used for the treatment of pulmonary arterial hypertension (PAH). The first ERA approved was bosentan, a dual ETA/ETB receptor antagonist, which demonstrated efficacy in improving exercise capacity and functional class in patients with PAH.9 Subsequently, ambrisentan, a selective ETA receptor antagonist, was introduced, offering improved hepatic safety compared with bosentan.9 Ambrisentan remains widely used, although adverse effects such as peripheral oedema, headache and palpitations have been commonly reported.10 Macitentan, another dual ERA, was later developed with enhanced tissue penetration and a longer half-life, offering improved receptor binding.11 The last ERA approved for PAH was sitaxsentan, another ETA-selective antagonist.12 However, due to reports of fatal hepatotoxicity, sitaxsentan was voluntarily withdrawn from the market in December 2010, and all clinical trials were halted.12
While ERAs have predominantly been utilized in PAH, they have also been explored for their potential in managing arterial hypertension. The drug darusentan, a selective ETA receptor antagonist with marginal ETB selectivity, demonstrated a BP reduction of ~10 mmHg during the DORADO trial (Phase 3, Randomized, Double-Blind, Placebo-Controlled, Multi-Center, Parallel Group Study to Evaluate the Efficacy and Safety of Fixed Doses of Darusentan in Subjects With Resistant Systolic Hypertension Receiving Combination Therapy With Three or More Antihypertensive Drugs, Including a Diuretic [Protocol DAR-311]; ClinicalTrials.gov identifier: NCT00330369).13 However, it ultimately did not meet the primary goals of the trial since it had a flat dose–response curve and a high incidence of adverse effects, which limited its clinical utility.13 In contrast, aprocitentan, an active metabolite of macitentan, represents a next-generation dual ERA with balanced antagonism of both ETA and ETB receptors.7,8 It has demonstrated consistent antihypertensive efficacy with a favourable safety profile, primarily characterized by mild, diuretic-responsive oedema, which supports its potential as a clinically promising treatment for rHTN. Table 1 compares the ERAs discussed above.7,8,13–21
Table 1: Comparison of endothelin receptor antagonists13–21
| ERA | Mechanism of action | Dosage (adults) | Key adverse effects | Special considerations |
| Bosentan | Dual ETA/ETB antagonist | Oral 62.5–125 mg BID | Transaminitis, mild anaemia, peripheral oedema, nausea, vomiting, palpitations, headache, decreased sperm count | Approved for PAH; monitor LFTs monthly; CYP3A4 interactions; teratogenic; biliary excretion, bio-transformation elimination |
| Ambrisentan | Selective ETA antagonist | Oral 5–10 mg QD | Less hepatotoxicity, peripheral oedema, mild anaemia, nasal congestion, headache | Approved for PAH; lower risk of liver injury; monitor for fluid retention; teratogenic; biliary excretion, bio-transformation elimination |
| Macitentan | Dual ETA/ETB antagonist (more ETA selective) | Oral 10 mg QD | Peripheral oedema, mild anaemia, nasopharyngitis, headache | Approved for PAH; used in CKD trials; lower hepatotoxicity risk; teratogenic; renal, faecal, bio-transformation elimination |
| Sitaxsentan (withdrawn) | Selective ETA antagonist | Oral 100 mg QD | Hepatotoxicity, peripheral oedema, nausea, headache | Approved for PAH; withdrawn due to fatal hepatotoxicity; renal, faecal elimination |
| Darusentan | Selective ETA antagonist | Oral 50–300 mg QD | Peripheral oedema, headache | Studied in rHTN trials but not approved; teratogenic; biliary excretion |
| Aprocitentan | Dual ETA/ETB antagonist | Oral 12.5 mg QD | Peripheral oedema, decrease in haemoglobin, potential decreased sperm count | Approved for rHTN; monitor for fluid retention; long half-life (~41 h); teratogenic; renal, faecal, bio-transformation elimination |
BID = twice daily; CKD = chronic kidney disease; CYP = cytochrome P450; ERA = endothelin receptor antagonist; ETA = endothelin A; ETB = endothelin B; LFT = liver function test; PAH = pulmonary arterial hypertension; QD = once daily; rHTN = resistant hypertension.
Pharmacological basis of aprocitentan
Aprocitentan is a dual ERA that inhibits the binding of ET-1 to both ETA and ETB receptor subtypes. Activation of the ETA receptor by ET-1 triggers a cascade of pathophysiological responses that raise intracellular calcium levels.18 This leads to vasoconstriction, smooth muscle contraction, cellular proliferation, endothelial dysfunction, vascular and cardiac remodelling, hypertrophy, sympathetic nervous system activation and increased aldosterone production.18 These effects collectively contribute to impaired sodium and water homeostasis in the kidneys, ultimately driving sustained elevations in BP and contributing to the pathogenesis of rHTN. Additionally, the presence of a sulfamide moiety in the aprocitentan structure indicates a potential secondary mechanism besides dual ERA, involving carbonic anhydrase inhibition.22 Many carbonic anhydrase isoforms are expressed in vascular smooth muscle cells and endothelial cells, playing a role in modulating vascular function.22 This potential additional mechanism of action may contribute synergistically to its antihypertensive effects, offering a broader therapeutic impact.
Pharmacokinetic studies have shown that aprocitentan exhibits similar plasma concentration–time profiles across single doses up to 600 mg and multiple daily doses up to 100 mg.18 Peak serum concentrations (C_max) occur between 3 and 9 h post-administration, with a prolonged elimination half-life (t_½) of approximately 44 h.18 The time to reach maximum concentration (Tmax) increases with higher doses, indicating dose-dependent absorption kinetics above 100 mg.18 Steady-state levels are attained after 8 days of once-daily dosing, with an approximate threefold drug accumulation.23 Aprocitentan is highly protein-bound (>99%), mainly to albumin, and this binding is unaffected by renal or hepatic impairment. Most of its BP-lowering effect occurs within the first 2 weeks of treatment.23
Metabolic profiling indicates that aprocitentan is predominantly eliminated through two cytochrome P450 (CYP)-independent pathways.18 It is done so through a metabolic profile that has a low potential for CYP-mediated drug–drug interaction, such as non-enzymatic hydrolysis to metabolite M1 (32%) and uridine diphosphate glucunosyltransferases (UGT)-mediated N-glucosidation to metabolite M3 (25%), primarily via UGT1A1 and UGT2B7.18 Following administration of a radiolabelled dose, approximately 52% of the compound is excreted in urine (with only 0.2% as unchanged drug) and 25% in faeces (6.8% as unchanged drug).18 These pharmacokinetic and metabolic characteristics support aprocitentan’s suitability for once-daily oral dosing and suggest a low risk of clinically significant drug–drug interactions.
First clinical trial of dual endothelin receptor antagonist for resistant hypertension
The Parallel-Group, Phase 3 Study with Aprocitentan in Subjects with Resistant Hypertension (PRECISION; Multi-center, Blinded, Randomized, Parallel-group, Phase 3 Study With Aprocitentan in Subjects With Resistant Hypertension [RHT]; ClinicalTrials.gov identifier: NCT03541174) trial was a multicentre, randomized, double-blind, placebo-controlled clinical trial that was designed to evaluate the safety and efficacy of aprocitentan in 730 patients with rHTN.24 This included a high-risk population with individuals of advanced age, many with CKD, diabetes and Black or African American race/ethnicity, which are groups disproportionately affected by rHTN and cardiovascular mortality. The trial consisted of three parts:
-
a 4-week double-blind phase where patients received aprocitentan (12.5 or 25 mg) or placebo;
-
a 32-week single-blind phase where all participants received aprocitentan 25 mg; and
-
a 12-week double-blind withdrawal phase with patients re-randomized to aprocitentan or placebo.24
The primary endpoint was the change in unattended office systolic blood pressure (SBP) from baseline to week 4, with key secondary endpoints including changes in sitting office diastolic blood pressure (DBP) and in ambulatory 24 h SBP and DBP from the start of withdrawal to week 40.24
Results showed a significant and sustained antihypertensive effect of aprocitentan both in office and in ambulatory settings. After 4 weeks, office SBP dropped by about 15 mmHg with aprocitentan versus 11.5 mmHg with placebo, a difference of roughly ~3.8 mmHg (p≈0.004).24 Meanwhile, DBP fell by ~4 mmHg versus placebo.24 These effects persisted through the 32-week treatment phase, and re-randomization to placebo in part 3 led to rapid increases in office SBP. Results from ambulatory BP monitoring were consistent with office findings throughout all three phases, confirming the drug’s efficacy in long-term BP control.24 Notably, the ambulatory BP effects were most pronounced during nighttime, with a higher SBP decrease observed.24 Side effects were found to be dose dependent, with lower doses of 12.5 mg still having a substantial BP effect with a lower side-effect profile.24 Overall, aprocitentan demonstrated significant and durable BP-lowering effects in high-risk populations with rHTN.24
Evaluating the indication, safety and side effects of aprocitentan
Following the PRECISION trial, aprocitentan was approved as a daily 12.5 mg oral medication taken once daily, with or without food. Although this article focuses on the role of aprocitentan in rHTN, aprocitentan is indicated for the treatment of hypertension in combination with other antihypertensive drugs, to lower BP in adult patients who are not adequately controlled on other drugs.23 Although it leads to incremental BP-lowering effects, the 25 mg dose was not approved over the 12.5 mg dose, given its association with a higher risk of adverse effects.23,24 Based on the current literature and the official US Food and Drug Administration (FDA) drug label, peripheral oedema is the most frequently reported adverse effect, particularly at higher doses. Notably, oedema was observed in 18% of patients receiving 25 mg, twice the approved dose of 12.5 mg, compared with 9% of those on the approved dose and only 2% in the placebo group.23 Importantly, aprocitentan has not been studied in patients with heart failure, New York Heart Association Stage III–IV, with unstable cardiac function or with a pro-brain natriuretic peptide (BNP) >500.23 Given the observed risk of fluid retention and the limited information on this medication in patients with this comorbidity, its use is not recommended in this population.23
Aprocitentan is contraindicated in pregnancy and should be avoided in women who may become pregnant, based on animal studies that demonstrated risk of foetal harm.23 Upon initial approval, the medication carried a boxed warning and was available only through the Risk Evaluation and Mitigation Strategies (REMS) programme. However, as of April 2025, the FDA removed the REMS requirement while still maintaining a strong warning regarding embryo-foetal toxicity, with drug benefits deemed to outweigh the risks.23 The embryo-foetal toxicity is attributed to the critical role of the ETA receptor in vascular and organ development; blocking this receptor may disrupt normal angiogenesis.23 Current FDA guidelines recommend the use of effective contraception for at least 1 month prior to starting therapy, throughout treatment and for 1 month following discontinuation.23 A pregnancy test should be performed prior to starting contraception, and if pregnancy occurs during treatment, the drug should be discontinued immediately. Additionally, breastfeeding is not recommended during therapy.22
Aprocitentan has also been associated with a decrease in haemoglobin levels, typically observed early in treatment but often stabilizing over time.23 A decrease of around 2 g/dL was observed in 7% of patients treated with 12.5 mg aprocitentan, versus 1% in those in the placebo group.23 As a precaution, haemoglobin should be assessed before initiation and monitored periodically throughout therapy. Its use is not recommended in patients with severe anaemia.22 Similarly to other agents in its class, aprocitentan may affect spermatogenesis and decrease sperm counts. In studies of male rats and dogs given very high doses, testicular changes such as seminiferous tubule dilation and tubular degeneration were observed.23 No adverse effects on sperm count, motility or morphology were observed at the tested dose up to almost 52-fold human exposure.23 However, given the decreased sperm count clinical risk identified with bosentan, a potential for clinical fertility risk with aprocitentan in males cannot be excluded, and it is currently unknown whether these effects are reversible.23
Although hepatotoxicity has been reported with this drug class, clinical trials with aprocitentan did not show elevations in liver function tests (LFTs). Nevertheless, LFTs should be assessed at baseline and monitored periodically during treatment.23 Therapy should not be initiated in patients with elevated transaminases, and liver function should be evaluated before starting treatment in those with hepatic impairment.23 No dose adjustment is necessary in patients with mild hepatic impairment (Child–Pugh Class A), but its use should be avoided in those with moderate-to-severe hepatic impairment (Child–Pugh Class B and C) due to an elevated risk of hepatotoxicity and poor clinical outcomes.23 In summary, aprocitentan is generally well tolerated, but its use requires consideration for specific safety concerns in certain populations. Further research is required to ascertain the drug’s long-term effects and its possible interactions with other antihypertensive treatments.24 Additionally, determining whether this drug reduces the overall burden of cardiovascular mortality and morbidity warrants further investigation to fully understand its potential clinical impact.24
Aprocitentan’s potential role in special populations: Chronic kidney disease, Black patients
The emerging role of aprocitentan as an agent in the treatment of rHTN carries important implications for specific patient populations, including those with comorbid conditions such as CKD. Aprocitentan has demonstrated significant antiproteinuric effects in patients with diabetes and CKD stages III and IV, including a 50% reduction in urinary albumin-to-creatinine ratio (UACR) by week 36 of treatment in part 2 of the trial.5 After 4 weeks of randomized withdrawal, UACR increased by 73% with placebo versus 14% with aprocitentan.5 These renal benefits are thought to stem from reduced intraglomerular pressure through post–glomerular vasodilation and decreased renal vascular hypertrophy, fibrosis and inflammation.25 ET-1 concentrations tend to rise as CKD advances, proving the therapeutic relevance of targeting the endothelin pathway in this population.25 ERAs have been studied in CKD for over a decade, with early evidence showing that selective ETA antagonism improves renal blood flow and reduces proteinuria, while ETB antagonism may cause renal vasoconstriction.26 In addition, studies in maintenance haemodialysis patients have found that higher baseline ET-1 levels correlate with elevated pre- and post-dialysis SBP and an increased risk of intradialytic hypertension.27 These findings highlight the therapeutic potential of aprocitentan for hypertension in patients with CKD, including those undergoing dialysis.
The long half-life and potential sympatholytic effects of aprocitentan also contribute to its pronounced impact on nocturnal BP, which holds prognostic value for Black patients who may experience higher rates of nighttime hypertension.5 The strong association between nocturnal BP and cardiovascular outcomes underscores the potential prognostic significance of the use of aprocitentan in this group. Notably, Black patients with hypertension may have disproportionately higher plasma and vascular concentrations of ET-1 compared with White individuals.5 They are more likely to exhibit salt-sensitive, low-renin hypertension, which is a phenotype closely linked to heightened endothelin activity.5 This pathway is also activated in patients prone to developing rHTN, suggesting that ERAs like aprocitentan may provide a more targeted and effective treatment approach in Black patients.
Aprocitentan and the 2025 AHA/ACC High Blood Pressure Guideline
Aprocitentan has been included in the 2025 AHA/ACC HBP Guideline in the section for rHTN, but its current classification and recommended use warrant clarification. Although originally denoted in guidelines as a potent vasodilator, aprocitentan may have unique properties when added as a fourth or fifth agent in rHTN.3 Unlike traditional vasodilators such as hydralazine or minoxidil, aprocitentan’s approved 12.5 mg dosage has not been linked to reactive tachycardia, orthostatic hypotension or headaches. Its antihypertensive effect is seen only in pathological states where the endothelin system is upregulated, as demonstrated in the PRECISION trial.3,9,23 Therefore, utilizing aprocitentan may not require concurrent use of a beta-blocker and loop diuretics as is seen with traditional vasodilators. In the PRECISION trial, aprocitentan was added to a background of a calcium channel blocker, a renin–angiotensin system inhibitor and hydrochlorothiazide, not a beta-blocker or loop diuretic.8 Its mechanism of action, which includes inhibition of endothelin-mediated effects such as vascular hypertrophy, fibrosis and neurohormonal activation, aligns it more closely with disease-modifying agents like macitentan than with simple vasodilators.11,18 While oedema and fluid retention are known side effects, the 2025 AHA/ACC HBP Guideline cited potential limitations of aprocitentan’s use due to the 9–18% incidence of this side effect.3 However, this combines data from both approved (12.5 mg, 9%) and unapproved (25 mg, 18%) doses; thus, the safety profile should be contextualized accordingly.9,23 Although not yet directly compared with spironolactone for effective BP lowering, aprocitentan represents a valuable alternative for patients intolerant to MRAs, offering a novel mechanism without the side effects typically associated with traditional vasodilators.
Conclusion
The treatment of rHTN represents a significant clinical and public health challenge, characterized by poor BP control despite optimal use of conventional antihypertensive therapies. The condition is closely associated with heightened cardiovascular risk, progression of CKD and a disproportionate effect on Black patients. Current antihypertensive therapies can fail to adequately control BP in these patients, underscoring the need for novel treatment options. Aprocitentan, a novel dual ERA, offers a new avenue for managing rHTN by targeting the underutilized endothelin pathway. Clinical evidence demonstrates aprocitentan’s sustained efficacy in lowering BP and improving vascular health in this patient population. With a favourable pharmacokinetic profile and once-daily oral dosing, aprocitentan may fill a critical gap in hypertension management and represent a viable new option for managing rHTN. Moreover, aprocitentan’s antiproteinuric effects and benefits in nocturnal BP control suggest added therapeutic value in patients with CKD and in Black patients. Nevertheless, clinicians should remain mindful of the drug’s safety profile, including risks of peripheral oedema, and contraindications during pregnancy and certain liver conditions. Aprocitentan represents a valuable addition to the therapeutic arsenal for rHTN, especially in patients who have not achieved adequate control, given the current knowledge of its pharmacology and clinical effects.







