Hypertension affects over 1.4 billion adults worldwide and remains the leading modifiable risk factor for global cardiovascular (CV) morbidity and mortality. It is responsible for an estimated 10.8 million deaths annually and contributes significantly to the global burden of ischaemic heart disease, stroke, heart failure and chronic kidney disease (CKD).1 Despite the availability of safe, effective antihypertensive therapies, a substantial proportion of patients exhibit persistent blood pressure (BP) elevation despite multi-drug treatment, a condition termed resistant hypertension (RH). This particularly challenging subset is often associated with poor BP control rates, high CV risk and substantial healthcare utilization. This comprehensive article examines the current understanding of RH from epidemiological patterns and pathophysiological mechanisms to diagnostic challenges and evolving therapeutic strategies. We critically evaluate the evidence base for contemporary management approaches and discuss future directions for improving outcomes in this high-risk patient population.
Definition and terminology
The American Heart Association (AHA) and the European Society of Hypertension (ESH) define RH as uncontrolled BP that remains elevated above goal despite adherence to an optimal triple-drug regimen that includes:
-
a renin–angiotensin–aldosterone system (RAAS) blocker (an angiotensin-converting enzyme [ACE] inhibitor or angiotensin receptor blocker)
-
a calcium channel blocker (CCB)
-
a thiazide/thiazide-like diuretic, wherein all agents have been administered at maximum or maximally tolerated doses and at the appropriate dosing frequency (Table 1).2,3
Table 1: Definition and terminologies concerning resistant hypertension2,3
| Term | Academic definition |
| RH | Persistent elevation of BP above guideline-recommended targets despite the use of ≥3 antihypertensive agents from different pharmacological classes – typically including a long-acting CCB, a RAAS blocker and a diuretic, administered at maximally tolerated or optimal doses. Diagnosis requires exclusion of pseudo-resistance |
| Pseudo-resistance | Apparent lack of BP control in a patient receiving ≥3 antihypertensive drugs, due to factors such as inaccurate BP measurement, the white-coat effect, inadequate dosing, clinical inertia or poor medication adherence rather than true pharmacological resistance |
| White-coat RH | Office BP remains above target despite ≥3 antihypertensives, but home or ambulatory BP monitoring shows controlled systolic and diastolic pressures |
| Controlled RH | Target BP is achieved but requires ≥4 antihypertensive agents at maximally tolerated doses |
| Apparent treatment RH | Used when adherence, dose adequacy or out-of-office BP data are unavailable, preventing distinction between true and pseudo-resistance |
| Clinical inertia | Failure to initiate, intensify or adjust therapy despite persistent uncontrolled BP, thereby delaying achievement of treatment goals |
| Refractory hypertension | Persistent uncontrolled BP despite treatment with ≥5 antihypertensive agents from different classes at near-maximal doses, including a long-acting thiazide-type diuretic (e.g. chlorthalidone) and an MRA (e.g. spironolactone) |
BP = blood pressure; CCB = calcium channel blocker; MRA = mineralocorticoid receptor antagonist; RAAS = renin–angiotensin–aldosterone system; RH = resistant hypertension.
Controlled RH refers to BP at target levels while receiving four or more agents, whereas refractory hypertension denotes uncontrolled BP despite ≥5 antihypertensives, including a diuretic and a mineralocorticoid receptor antagonist (MRA).2 The term RH includes both the subset of patients with hypertension, wherein BP is either controlled or uncontrolled, depending on the number of antihypertensive agents used. Patients with difficult-to-treat hypertension are often referred to as patients with ‘resistant’ or ‘refractory’ hypertension.2 Until recently, refractory hypertension was not historically differentiated from RH. Refractory hypertension, an extreme phenotype of antihypertensive treatment failure, has been defined as hypertension uncontrolled with the use of five or more antihypertensive agents, including a long-acting thiazide diuretic and an MRA.4
Epidemiology
RH represents a significant global health problem, with estimates suggesting that between 100 and 500 million individuals worldwide may be affected.2 This wide range reflects differences in diagnostic criteria, study methodologies and population characteristics across regions. In a comprehensive meta-analysis that included 91 cohort and cross-sectional studies involving more than 3.2 million patients with hypertension, the prevalence of RH was estimated to be approximately 10%.5 Data suggest that the prevalence of RH is around 8.5–20% among US adults with hypertension.6–8 Insights from the largest analysis of patients with RH (Cardiovascular Quality Improvement and Care Innovation Consortium [CV-QUIC]) reported a prevalence of RH to be 8.5% using the contemporary BP cutoff of 130/80 mmHg.7 Contemporary data from the National Health and Nutrition Examination Survey (NHANES) found that 15.9% of adult patients with hypertension met the criteria for RH, highlighting the widespread impact of this entity.9 The burden of RH is particularly pronounced in low- and middle-income countries, where the prevalence of hypertension is rising rapidly and control rates remain suboptimal. Data from the Jaipur Heart Watch study in India reported the prevalence of RH to be 19.4%.10
RH is more common among older adults, males, individuals of African ancestry and those with comorbid metabolic syndromes or CKD. Data from the Research Action for Health Network (REACHnet) reported that patients with RH had a significantly higher prevalence of diabetes, dyslipidaemia, coronary artery disease, stroke, heart failure with preserved ejection fraction, heart failure with reduced ejection fraction, myocardial infarction (MI), CKD, sleep apnoea and other comorbidities when compared with patients with controlled hypertension.8 RH carries a significant clinical burden, as these patients are at greater risk for target-organ damage, including left ventricular hypertrophy, diastolic dysfunction, carotid intimal–medial thickening and microalbuminuria.11 Patients with RH have a twofold increased risk of CV disease events compared with patients whose hypertension is responsive to treatment. Longitudinal cohort studies demonstrate that RH confers an elevated risk of MI (hazard ratio [HR]: 1.47), stroke (HR: 1.42), heart failure (HR: 1.70) and all-cause mortality (HR: 1.33) compared with controlled hypertension.12 RH significantly accelerates renal decline, conferring an increased risk for advanced CKD and nearly doubling the likelihood of progressing to end-stage renal disease.13 The burden of RH extends beyond individual patients to healthcare systems, with increased rates of hospitalizations, healthcare utilization and medication costs.14 Effective identification and management of RH is, therefore, a public health priority.
Pathophysiology
RH represents the convergence of multiple interacting mechanisms that sustain BP elevation despite optimized pharmacological therapy. Rather than a single pathway, RH reflects the interplay of sympathetic nervous system (SNS) overactivity, RAAS dysregulation, sodium retention, vascular remodelling, renal impairment, metabolic abnormalities and inflammatory processes (Figure 1).15 One of the most consistent features of RH is SNS overactivity. Heightened sympathetic tone in RH raises BP through peripheral vasoconstriction, increased cardiac output and enhanced renal sodium reabsorption. In addition, it stimulates renin release, thereby linking neural activation with RAAS pathways.16 Clinical conditions with sympathetic overactivity, such as obesity, obstructive sleep apnoea (OSA) and CKD, are all overrepresented in RH cohorts. The therapeutic relevance of this mechanism is underscored by the observation that sympatholytic drugs, such as clonidine, and more recently catheter–based renal denervation (RDN), can lower BP in the subsets of patients with true RH.
Figure 1: Pathophysiological mechanisms of resistant hypertension
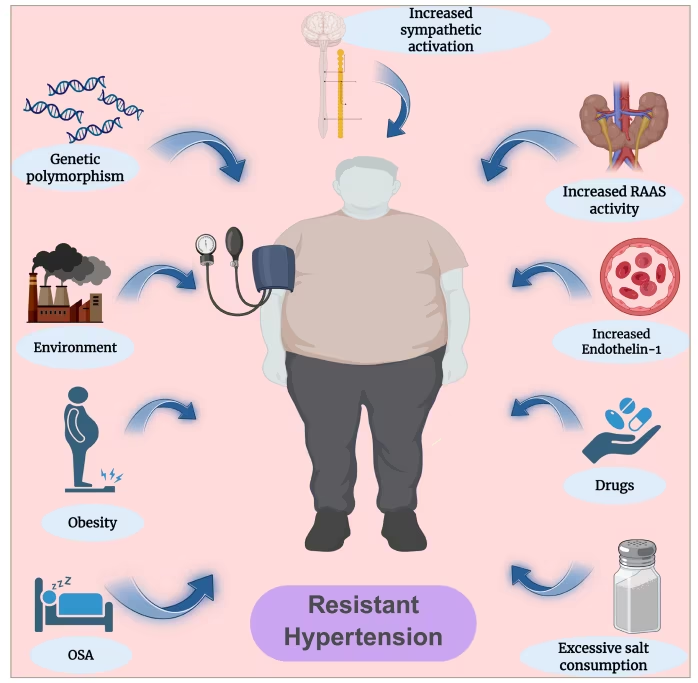
Schematic representation of the major mechanisms contributing to RH. Neurohormonal activation includes increased sympathetic activity, RAAS dysregulation and endothelin-1 upregulation. Metabolic and lifestyle contributors include obesity, OSA and excessive dietary salt intake. Environmental and pharmacological influences include exposure to certain drugs and environmental stressors. Genetic predisposition also plays a role. Together, these interconnected pathways perpetuate elevated BP despite multidrug therapy. Created with BioRender.com.
BP = blood pressure; OSA = obstructive sleep apnoea; RAAS = renin–angiotensin–aldosterone system; RH = resistant hypertension.
A second central pathway for RH is RAAS dysregulation, in particular aldosterone excess. Aldosterone promotes sodium retention, volume expansion, vascular remodelling and cardiac and renal fibrosis. Primary hyperaldosteronism, once considered rare, is now recognized in up to one-fifth of patients with RH.17 Even in the absence of overt primary aldosteronism, inappropriate aldosterone secretion is common in this group. The clinical relevance is clear: MRAs, particularly spironolactone, have been shown to consistently produce substantial BP reductions in RH. Closely linked to RAAS activation is sodium retention and volume expansion. High dietary salt intake, impaired renal sodium excretion and increased sodium sensitivity all contribute to RH development. Salt sensitivity is particularly prevalent in individuals of African and South Asian ancestry, who display exaggerated BP responses to sodium loading.18 CKD exacerbates this process by reducing natriuretic capacity, leading to extracellular fluid accumulation and resistant BP. Clinical studies have shown that strict sodium restriction (<100 mmol/day) can lower systolic BP in patients with RH, underlining the centrality of salt in disease expression. In parallel, structural and functional vascular changes perpetuate hypertension. Patients with RH often demonstrate endothelial dysfunction, impaired nitric oxide bioavailability and increased oxidative stress, all of which limit vasodilatory capacity. These vascular alterations both raise BP and blunt the efficacy of antihypertensive therapy, creating a cycle of persistent resistance. Renal contributions extend beyond sodium retention. CKD, a major driver of RH, has a prevalence reaching 30–40% in this population. Reduced nephron mass, glomerulosclerosis and interstitial fibrosis impair renal autoregulation, further elevating BP. Renal ischaemia, whether macrovascular (atherosclerotic renal artery stenosis [RAS]) or microvascular (rarefaction), contributes to chronic activation of neurohormonal pathways. Importantly, hypertension and kidney disease exist in a reciprocal relationship: RH accelerates CKD progression, while CKD worsens hypertension.19
OSA represents another critical factor and is present in up to 70–80% of patients with RH.20 OSA drives BP elevation through intermittent hypoxemia, sympathetic surges, oxidative stress and RAAS activation.20 Negative intrathoracic pressure swings during apnoeic episodes increase cardiac afterload, while nocturnal BP non-dipping is characteristic. Obesity and metabolic disturbances are tightly linked to RH. Obesity increases sympathetic activity, enhances renal sodium reabsorption and promotes volume expansion. Adipose tissue-derived adipokines, including leptin, angiotensinogen and pro-inflammatory cytokines, contribute to vascular dysfunction and insulin resistance.21 Metabolic syndrome and type 2 diabetes further exacerbate RH through endothelial dysfunction, oxidative stress and arterial stiffness. Emerging evidence implicates immune and inflammatory pathways in RH. Animal studies have demonstrated infiltration of T lymphocytes and macrophages into the kidney and vasculature, where they release cytokines such as interleukin-6 and tumour necrosis factor-alpha.22 These mediators promote sodium retention, vascular remodelling and heightened sympathetic activity. The association of RH with inflammatory comorbidities, including obesity, diabetes and CKD, supports an immunoinflammatory paradigm.23 In reality, RH almost never results from a single mechanism. Instead, multiple interdependent processes sustain elevated BP. This integrated model (Figure 1) explains why RH is difficult to control with standard therapy and why multimodal approaches, encompassing lifestyle measures, targeted pharmacotherapy and device-based interventions, are required for effective management.
Diagnostic approach
Exclusion of pseudo-resistant hypertension
Prior to establishing a diagnosis of RH, it is prudent to exclude pseudo-RH. The most common causes include inaccurate BP measurement, such as the use of an incorrect cuff size, faulty devices or the presence of significant brachial artery calcification (Osler’s sign), which may render the artery incompressible.2 Secondly, the ‘white-coat effect’, wherein BP is elevated in the clinical setting but not in ambulatory or home readings, is present in 20–30% of patients with apparent RH and often requires 24 h ambulatory BP monitoring (ABPM) to exclude the white-coat effect.2 Nonadherence to prescribed antihypertensive therapy is one of the most important and frequently overlooked contributors to RH. Reported prevalence varies widely in the published literature, ranging from 5% to 80%, depending on the population studied, definitions used and methodology employed to assess adherence.24 Clinicians play a crucial role in reinforcing the importance of adherence, addressing barriers such as polypharmacy, complex regimens and medication side effects. The usage of dosette boxes and polypills has previously been shown to improve adherence. More objective measures to assess compliance with antihypertensive medications include pharmacy fill histories, pill counts, directly observed therapy or antihypertensive drug urine screening, although these are not universally available and are limited to specialist settings. Other contributing factors include the use of concurrent medications (e.g. non-steroidal anti-inflammatory drugs, oral contraceptives, sympathomimetics), over-the-counter preparations (e.g. decongestants, herbal remedies) and recreational substances. Identification and correction of these factors can prevent misclassification of patients as having RH and avoid unnecessary escalation of therapy.
In patients with apparent treatment-RH, the first step is to systematically exclude pseudo-resistance. This four–step approach (Figure 2) requires:
-
standardized office BP measurement using an automated cuff;
-
confirmation of adherence to antihypertensive therapy;
-
exclusion of drug- or substance-induced hypertension;
-
out-of-office BP monitoring: 24 h ABPM is the gold standard to detect white-coat or masked hypertension. If ABPM is unavailable, home BP monitoring with validated devices and standardized protocols is recommended.1
Figure 2: Diagnostic pathway for confirming true resistant hypertension
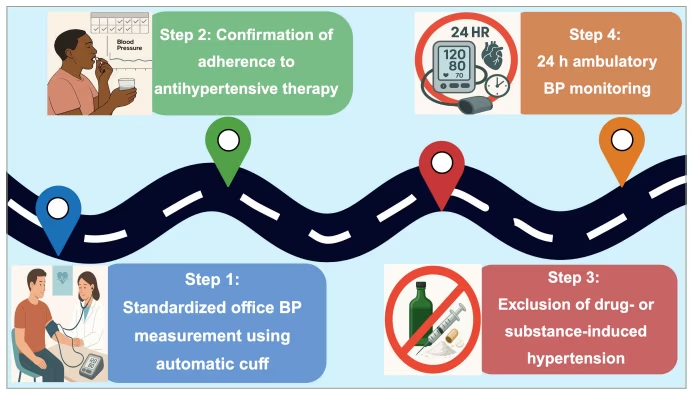
Created with BioRender.com
BP = blood pressure.
Evaluate for secondary hypertension
A significant proportion of RH is attributable to underlying secondary causes (Table 2).5,25–30 Failure to identify and treat these causes is a major reason for apparent treatment resistance.31
Table 2: Secondary causes of hypertension associated with resistant hypertension5,25–30
| Category | Clinical condition | Prevalence in RH (%) | Clinical features | Diagnostic modality | Preferred therapy |
| Sleep-related | Obstructive sleep apnoea | 50–7025 | Snoring, excessive daytime sleepiness, obesity | Polysomnography | CPAP, weight reduction |
| Renal | Chronic kidney disease | 10.3–22.95 | Elevated creatinine, proteinuria | Serum creatinine, eGFR, urinalysis, USG abdomen | Treat underlying disease, RAAS blockade |
| Renal artery stenosis | 5–2026 | Abdominal bruit, sudden hypertension worsening | Duplex Doppler, CT/MR angiography | Optimal medical therapy ± revascularization | |
| Endocrine | Primary aldosteronism | 8–2027 | Hypokalaemia, adrenal mass | ARR, confirmatory suppression test | Spironolactone/eplerenone; adrenalectomy if unilateral |
| Phaeochromocytoma | <128 | Headaches, sweating, palpitations | Plasma-free metanephrines, | Surgery ± targeted therapy | |
| Thyroid disease | <129 | Weight changes, heat/cold intolerance | TSH, free T4, free T3 | Thyroid-specific therapy | |
| Drug/substance | NSAIDs, alcohol, etc. | 2–530 | Medication/alcohol history | Detailed history | Discontinue/substitute agent |
ARR = aldosterone-to-renin ratio; CPAP = continuous positive airway pressure; CT = computed tomography; eGFR = estimated glomerular filtration rate; MR = magnetic resonance; NSAIDs = non-steroidal anti-inflammatory drugs; RAAS = renin–angiotensin–aldosterone system; RH = resistant hypertension; T3 = triiodothyronine; T4 = thyroxine; TSH = thyroid-stimulating hormone; USG = ultrasound.
-
Primary aldosteronism: its prevalence in RH populations is high, estimated at 15–20% and is characterized by autonomous aldosterone production, leading to sodium retention, potassium wasting and hypertension that is often resistant to standard therapy. It requires screening with the morning aldosterone-to-renin ratio (ARR) while correcting hypokalaemia and reviewing interfering medications. Confirmation and subtype testing (computed tomography [CT]/adrenal venous sampling) follow, with treatment being surgical in cases of unilateral adenoma, while patients with bilateral hyperplasia require therapy with MRAs.32
-
Renal parenchymal disease/CKD: CKD contributes to hypertension through multiple mechanisms: volume overload, RAAS activation and increased SNS activity. Renal parenchymal disease is suggested by elevated serum creatinine, abnormal urinalysis with proteinuria or haematuria and a known history of CKD. Workup includes measurement of serum creatinine, estimated glomerular filtration rate (eGFR), urinalysis, urine albumin-to-creatinine ratio and renal ultrasound for structural abnormalities.2,31
-
RAS: atherosclerotic RAS can lead to renovascular hypertension via RAAS activation. While its prevalence has declined with effective statin therapy, it should be considered, especially in patients with widespread atherosclerosis, flash pulmonary oedema, abdominal bruit or rapidly declining renal function. Contemporary trials (CORAL [Cardiovascular Outcomes in Renal Atherosclerotic Lesions] trial and ASTRAL [Angioplasty and Stenting for Renal Artery Lesions] trial) did not show outcome benefit of routine stenting over optimized medical therapy; however, revascularization (Figure 3A and B) is reserved for select high-risk phenotypes (e.g. recurrent flash pulmonary oedema or rapid loss of kidney function with high-grade bilateral disease/solitary kidney).33,34
-
OSA: it is highly prevalent in RH, with a strong bidirectional relationship between OSA and hypertension. Intermittent hypoxia and hypercapnia during apnoeic episodes lead to intense SNS activation, endothelial dysfunction, inflammation, oxidative stress and RAAS stimulation. It is strongly associated with obesity, loud snoring, witnessed apnoeas, excessive daytime sleepiness and increased neck circumference. Diagnosis requires formal polysomnography, although screening questionnaires, such as STOP-BANG, can help identify high-risk individuals. Continuous positive airway pressure therapy modestly reduces BP and improves overall CV outcomes in these patients.25
-
Phaeochromocytoma/paraganglioma: these are rare but life-threatening causes of catecholamine excess, leading to severe, often paroxysmal, hypertension. They often present with episodic headache, diaphoresis and tachycardia and are best screened using normetanephrine, plasma-free metanephrines or 24 h urinary fractionated metanephrines. Normetanephrine and metanephrine levels three-times or higher than the upper limit of normal are highly suggestive of phaeochromocytoma. If screening is positive, further imaging with abdominal/adrenal magnetic resonance imaging (MRI) or CT (Figure 3C and D) is indicated.28
-
Other causes: Cushing syndrome should be suspected in patients with central obesity, glucose intolerance, purple striae and proximal myopathy, with biochemical confirmation using 24 h urinary cortisol or dexamethasone suppression tests. Thyroid disorders can produce both systolic and diastolic hypertension, necessitating routine measurement of thyroid-stimulating hormone and free thyroxine, while hyperparathyroidism may contribute through hypercalcaemia and renal impairment, warranting serum calcium and parathyroid hormone testing.29 Other, less frequent causes include aortic coarctation (Figure 3E and F), which should be suspected in younger individuals with radio-femoral delay or discrepant BP between the upper and lower limbs.
Figure 3: Imaging spectrum of secondary hypertension
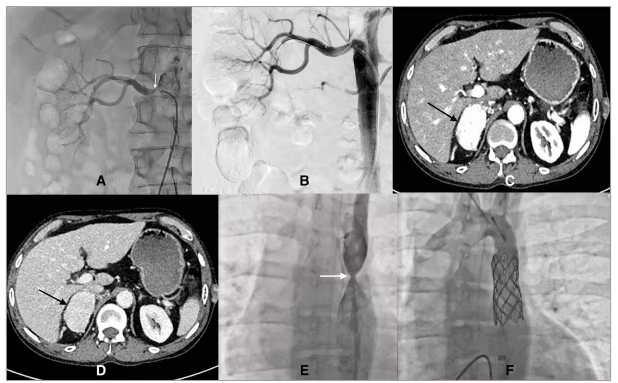
A, B: Renal angiography images demonstrating percutaneous transluminal renal artery stenting. (A) Pre-intervention angiogram shows a critical stenosis at the ostium of the right renal artery (white arrow). (B) Post-stenting angiogram demonstrates successful deployment of the stent with restoration of vessel patency and improved perfusion of the renal parenchyma. C, D: CECT images in arterial (C) and venous (D) phases showing a well-defined, heterogeneously enhancing mass arising from the right adrenal gland (black arrow). The lesion demonstrates intense enhancement during the arterial phase with persistent heterogeneous enhancement on the venous phase, without invasion of adjacent structures. These features are characteristic of a right adrenal phaeochromocytoma. E, F: Aortogram showing severe focal coarctation of the descending thoracic aorta (white arrow) with post-stenotic dilatation (E). Following deployment of a covered stent across the coarctation segment, post-procedure angiogram demonstrates complete relief of the narrowing with good stent apposition and restoration of normal aortic calibre (F).
CECT = contrast-enhanced computed tomography.
Diagnostic workup for true resistant hypertension
Once pseudo-resistance is addressed, a focused evaluation for secondary causes and contributing factors should be initiated.
Step 1: Comprehensive history and physical examination
-
History: a meticulous history is essential, with particular attention to the patient’s complete medication list, including prescribed agents, over-the-counter drugs and herbal or dietary supplements. Assessment of adherence should be undertaken sensitively, and lifestyle factors, such as dietary sodium intake, alcohol consumption, physical activity and sleep quality, must be reviewed. Specific symptoms may suggest secondary aetiologies, such as muscle weakness or recurrent hypokalaemia in primary aldosteronism, or snoring and excessive daytime somnolence in OSA.
-
Physical examination: it should include measurement of BP in both arms to identify subclavian stenosis, careful cardiac and abdominal auscultation for bruits, evaluation for signs of volume overload and evaluation for clinical features of endocrine disorders, such as Cushing’s syndrome or thyroid disorders. Peripheral pulse assessment may also suggest vascular disease, including coarctation or peripheral arterial disease.
Step 2: Laboratory and basic diagnostic testing
-
Basic metabolic panel: this includes determination of serum sodium, potassium and creatinine (for eGFR) levels. Hypokalaemia, whether spontaneous or diuretic-induced, raises suspicion for primary aldosteronism.
-
ARR: this is the primary screening test for primary aldosteronism and should be performed after correcting hypokalaemia and, if possible, off interfering medications (particularly MRAs, which must be stopped for at least 6 weeks). An ARR of 20 or higher, with an aldosterone level of at least 15 ng/dL, warrants a confirmatory test (intravenous or oral salt-loading test).35 However, patients with clear signs, such as very low renin, hypokalaemia and high aldosterone, can often skip confirmation and go straight to adrenal imaging.
-
Urine studies: a 24 h urine collection for sodium, potassium and creatinine helps assess dietary sodium intake and the adequacy of diuretic therapy. Persistently high urinary sodium, despite counselling, suggests dietary non-adherence. A 24 h urinary metanephrines should be measured if phaeochromocytoma or paraganglioma is suspected. Additionally, the urine albumin-to-creatinine ratio provides valuable information about target organ damage and early nephropathy.36
-
Hormonal assays: these should be guided by clinical suspicion. Thyroid function tests are indicated in unexplained BP variability, while plasma-free metanephrines are especially indicated in the context of labile hypertension accompanied by headaches, palpitations and diaphoresis.32
-
Sleep study (polysomnography): this should be considered in patients with a high pre-test probability of OSA, identified by symptoms such as habitual snoring, witnessed apnoeas or excessive daytime sleepiness, particularly in individuals with obesity and a large neck circumference.25
Step 3: Advanced imaging
-
Renal artery duplex ultrasound: this provides a non-invasive initial screen for haemodynamically significant RAS.
-
Adrenal CT scan: if ARR is elevated, a thin-section CT of the adrenals is performed to identify an adenoma or hyperplasia.
-
Echocardiography: used to evaluate for left ventricular hypertrophy and diastolic dysfunction, which are markers of target organ damage and provide prognostic information.
Management strategies
A multifactorial approach is often needed to treat RH, and it includes a combination of lifestyle modification, pharmacotherapy and managing underlying comorbid conditions.
Lifestyle modification
Lifestyle changes play an integral part in the management of RH and should be implemented alongside appropriate pharmacological therapy. Regular physical activity has been consistently shown to lower BP across diverse populations, and emerging evidence supports its role specifically in RH. Both aerobic and resistance training appear beneficial, producing meaningful reductions in systolic and diastolic BP.2 Data from the TRIUMPH (Treating Resistant Hypertension Using Lifestyle Modification to Promote Health; ClinicalTrials.gov identifier: NCT02342808) trial suggested that both diet and exercise can lower BP in patients with RH. Findings of the study revealed that a 4-month structured programme comprising diet and exercise as adjunctive therapy resulted in significant reductions in both clinic and ambulatory BP in RH.37 Similarly, the EnRicH (The Role of Exercise Training in the Treatment of Resistant Hypertension; ClinicalTrials.gov identifier: NCT03090529) trial, which tested a 12-week programme of moderate-intensity aerobic exercise, demonstrated reductions of 7.1 mmHg in systolic and 5.7 mmHg in diastolic ambulatory BP, providing further evidence that exercise training can improve outcomes in RH.38 The current American College of Cardiology (ACC)/AHA 2025 guidelines recommend increasing physical activity through a structured exercise programme that includes aerobic exercise of at least 90–150 min per week for BP control.1
Dietary modifications in patients with hypertension include the Dietary Approaches to Stop Hypertension (DASH) diet along with sodium restriction. Currently, no DASH diet trials have been performed in the RH subset. However, the DASH diet has broader CV benefits beyond BP reduction. Improvements in lipid profiles, insulin sensitivity and endothelial function have been observed, which may be particularly advantageous given the clustering of cardiometabolic risk factors in patients with RH.39 Direct interventional evidence supporting sodium restriction in RH remains limited. In a small pilot study of 15 patients with confirmed RH, self-administered dietary sodium restriction over 2 weeks resulted in significant reductions in office BP, as well as urinary sodium excretion, suggesting that even short-term restriction may confer measurable benefit.40 Similarly, in a randomized control trial (RCT) evaluating dietary salt manipulation, a low-sodium diet was associated with substantial reductions in office systolic and diastolic BP (-22.7 and -9.1 mmHg, respectively). However, this trial was limited by its modest sample size, lack of blinding and short duration of intervention, raising concerns about generalizability.41 The 2025 ACC/AHA guidelines on high BP recommend a reduction in dietary sodium intake to <2,300 mg/day and moving towards an ideal limit of <1,500 mg/day to prevent or treat hypertension.1 Observational evidence consistently shows that diets rich in natural potassium sources, such as fruits, vegetables, legumes and juices, are associated with lower BP and reduced risks of stroke and mortality. The BP response appears dose-dependent: maximal benefit occurs at around 30 mmol/day of supplemental potassium, while doses >80 mmol/day may paradoxically increase BP, especially among patients taking antihypertensive therapy. As per the 2025 ACC/AHA guidelines on high BP, moderate potassium supplementation (3,500–5,000 mg/day) is recommended, with careful monitoring in individuals with CKD, those on RAAS blockade, or those at risk of hyperkalaemia.1
Weight loss has been proposed as a cornerstone intervention in the management of RH. Weight reduction can provide an average BP reduction of about 5 mmHg in hypertensive overweight adults.2 However, direct evidence evaluating its effects specifically in patients with RH remains limited. Pharmacological weight reduction strategies have shown promise. Glucagon-like peptide-1 receptor agonists, which are increasingly used in the management of obesity and type 2 diabetes, have been associated with modest reductions in BP and improvements in overall CV risk profile in patients with diabetes or established CV disease. More robust evidence comes from surgical interventions. In a sub-analysis of the GATEWAY (GAstric bypass to Treat obEse Patients With steAdy hYpertension; ClinicalTrials.gov identifier: NCT01784848) trial, which included patients with obesity and hypertension, the prevalence of RH significantly decreased following randomization to bariatric surgery compared with medical therapy.42 Interestingly, reductions in BP were observed early after surgery, preceding significant weight loss. This temporal relationship implies that mechanisms beyond pure weight reduction, such as improvements in sympathetic overactivity, restoration of sodium and water homeostasis, enhanced insulin sensitivity and attenuation of systemic inflammation, contribute to the observed antihypertensive effects.
Excess alcohol intake is a well-established contributor to elevated BP and is independently associated with RH.2 Reduction or cessation of alcohol consumption leads to meaningful BP reductions, often within weeks. Current ACC/AHA 2025 guidelines recommend that adults who currently consume alcohol should be advised to pursue abstinence, or at least reduce alcohol intake to ≤1 drink per day for women and ≤2 drinks per day for men.1 Stress management does form an integral component of BP control. Meditation, breathing control and yoga appear to be the most effective stress reduction strategies for BP control. The 2025 ACC/AHA guidelines recommend transcendental meditation training by a professional, followed by 2×20 min sessions per day while seated comfortably with eyes closed.1
Pharmacological management
As per the European Society of Cardiology (ESC) 2024, ESH 2024 and 2025 AHA/ACC guidelines, five main classes of drugs (Table 3) are recommended as first-line pharmacological treatments for hypertension: ACE inhibitors, angiotensin II receptor blockers (ARBs), CCBs, thiazide or thiazide-like diuretics and beta-blockers (BBs).1,43,44 The 2024 ESC guidelines on hypertension management recommend ACE inhibitors, ARBs, CCBs and thiazide or thiazide-like diuretics as preferred first-line antihypertensive agents, owing to their proven efficacy.43 Additionally, the guidelines emphasize the use of combination therapy as the initial pharmacological strategy in most patients, reflecting evidence that such an approach enhances BP control and improves clinical outcomes. Use of single-pill combination (SPC) therapy is strongly recommended to improve adherence, simplify treatment and achieve faster BP control – critical factors in RH. SPCs reduce pill burden, minimize therapeutic inertia and enhance long-term persistence with therapy. Current guidelines, including the 2025 AHA/ACC, endorse SPCs as the preferred strategy for initiating and intensifying antihypertensive therapy, particularly combinations incorporating a RAAS inhibitor + CCB + thiazide-type diuretic.1 In people with apparent or true RH, routine use of SPCs increases the likelihood of reaching target BP and reduces treatment gaps arising from multi-tablet regimens. The 2025 ACC/AHA guidelines recommend starting treatment preferentially with a combination of ACE inhibitors with CCBs or ACE inhibitors with thiazide/thiazide-like diuretics.1
Table 3: Adverse effects and monitoring for antihypertensive drug classes1
| Class | Class-specific adverse effects1 | Key monitoring |
| ACEi/ARB | ACEi: cough, hyperkalaemia, angioedema. ARB: hyperkalaemia | Monitor serum creatinine and potassium 1–2 weeks after initiating or adjusting therapy |
| DHP-CCB | Dihydropyridine calcium channel blocker: lower extremity oedema, gingival hyperplasia | Monitor for peripheral oedema; check heart rate |
| Thiazide-like diuretics | Hyponatraemia, hypokalaemia, volume depletion, renal dysfunction, glucose intolerance, diabetes mellitus, hyperuricaemia, gout | Monitor serum sodium, potassium and uric acid levels |
| Loop diuretic (eGFR <30 mL/min) | Hypokalaemia, volume depletion, renal dysfunction | Monitor electrolytes (Na+, K+) and volume status |
| MRA | Hyperkalaemia, volume depletion, renal dysfunction, gynaecomastia (spironolactone) | Monitor serum potassium and creatinine at 1 and 4 weeks after initiation or dose change, then every 3 months |
| Potassium-sparing diuretic | Hyperkalaemia, volume depletion, renal dysfunction | Monitor serum potassium and creatinine |
| Beta-blockers (vasodilating) | Bradycardia, heart block, bronchospasm, fatigue, depression | Nebivolol: monitor heart rate and blood pressure; watch for fatigue. (Beta-1 selectivity may benefit patients with asthma or COPD.) Carvedilol: monitor heart rate, blood pressure and body weight; watch for bradycardia and orthostatic hypotension |
| Alpha-1 antagonist | Nasal congestion, dizziness, orthostatic hypotension | Risk of first-dose syncope – give initial dose at bedtime. Monitor for orthostatic hypotension and dizziness |
| Centrally acting alpha-2 agonist | Drowsiness, orthostatic hypotension, depression | Common side effects include sedation and dry mouth. Caution: rebound hypertension can occur if stopped abruptly |
| Direct vasodilator | Reflex tachycardia, lower extremity oedema, drug-induced lupus (hydralazine) | Monitor for tachycardia (often co-administer with a beta-blocker), lupus-like syndrome (periodically check ANA), headaches and fluid retention |
| Emerging pharmacological therapies | ||
| ASIs | Hyperkalaemia, renal dysfunction | Monitor serum potassium (risk of hyperkalaemia), serum creatinine/eGFR, blood pressure response and assess for symptoms of adrenal insufficiency (rare) |
| Endothelin receptor antagonists | Oedema, headache, anaemia | Monitor body weight and peripheral oedema, haemoglobin/haematocrit (risk of anaemia), liver function tests (ALT/AST) and blood pressure response |
| siRNA-based RAAS inhibitors | Hyperkalaemia, injection-site reactions | Monitor serum potassium and renal function |
ACEi = angiotensin-converting enzyme inhibitor; ALT/AST = alanine aminotransferase/ aspartate aminotransferase; ANA = antinuclear antibody; ARB = angiotensin II receptor blocker; ASIs = aldosterone synthase inhibitors; COPD = chronic obstructive pulmonary disease; DHP-CCB = dihydropyridine calcium channel blocker; eGFR = estimated glomerular filtration rate; K+ = potassium; MRA = mineralocorticoid receptor antagonist; Na+ = sodium; RAAS = renin–angiotensin–aldosterone system; siRNA = small interfering RNA.
First principles: build the right base – the six-step approach:
-
Step 1: Optimization of the three-drug regimen: A rational triple-drug regimen usually combines:
-
an ACE inhibitor (e.g. ramipril) or ARB (e.g. telmisartan)
-
a long-acting dihydropyridine CCB (e.g. amlodipine)
-
a thiazide-like diuretic (e.g. chlorthalidone or indapamide).
-
An important cornerstone in managing RH is adjusting the diuretic therapy, as RH is often attributed to salt and water retention leading to volume overload, high sympathetic tone or a combination of these. Among the diuretic therapies, thiazide, thiazide-like and loop diuretics such as torsemide have proven antihypertensive effects.2
-
Step 2: Substitute optimally dosed thiazide-like diuretics: thiazide-like diuretics, such as chlorthalidone and indapamide, which have longer half-lives than hydrochlorothiazide, tend to be more effective antihypertensives. Comparative studies have reported a greater systolic blood pressure (SBP) reduction of 7–8 mmHg following switching to the same daily dose of chlorthalidone from hydrochlorothiazide.45 Similar evidence from multiple trials and meta-analyses has demonstrated a sustained and greater antihypertensive effect with thiazide-like diuretics, such as indapamide and chlorthalidone, when compared with hydrochlorothiazide.46 Another major issue with hydrochlorothiazide is that it loses its ability to induce predictable natriuresis when eGFR is <45 mL/min/1.73 m2 and thereby needs to be switched to a longer acting thiazide-like diuretic. If patients have an eGFR <30 mL/min/1.73 m2, indapamide should not be used; however, chlorthalidone remains effective in such patients.45 This was evident in the CLICK (Chlorthalidone in Chronic Kidney Disease; ClinicalTrials.gov identifier: NCT02841280) trial, wherein significant reductions in ambulatory and office BP were observed with chlorthalidone, independent of loop diuretic use, in patients with uncontrolled hypertension and stage IV CKD (eGFR: 15–29 mL/min/1.73 m2).47 With further decline in GFR, thiazide diuretics may be replaced by loop diuretics (e.g. furosemide, bumetanide or torsemide).
-
Step 3: Fourth drug of choice: an MRA: the PATHWAY-2 trial (Optimum Treatment for Drug-Resistant Hypertension; ClinicalTrials.gov identifier: NCT02369081) established spironolactone’s (25–50 mg/day) superiority over bisoprolol (5–10 mg daily) or doxazosin (5–10 mg daily) as an add-on therapy for RH. Around 60% of patients in the trial achieved BP control (home-based SBP: <135 mmHg) within 3 months. The largest reductions in SBP were seen in those with low renin levels, consistent with aldosterone excess driving resistance.48 Similarly, in the ReHOT (Resistant Hypertension Optimal Treatment; ClinicalTrials.gov identifier: NCT01643434) trial, which compared spironolactone (12.5–50 mg QD [once daily]) with clonidine (0.1–1–0.3 mg BID [twice daily]) as the fourth drug for RH, patients receiving spironolactone had greater reductions in 24 h systolic and diastolic BP and diastolic daytime ambulatory BP compared with clonidine.49 Further evidence in the form of a network meta-analysis involving about 3,000 individuals reported spironolactone to be the most effective treatment to reduce office SBP (-13.30 mmHg) and 24 h SBP (-8.46 mmHg) in RH.50 It is often prudent to start spironolactone at low doses (12.5–25 mg/day), thereby titrating to effect, along with monitoring of potassium/creatinine levels. The 2025 AHA guidelines recommend that, in adults with RH despite optimal treatment with first-line antihypertensive therapy and with an eGFR of ≥45 mL/min/1.73 m2), addition of an MRA is recommended to control BP (Class I, level of recommendation [LOR]: B).1 One of the major limitations of spironolactone is the risk of hyperkalaemia, especially in patients with CKD receiving RAAS blockers. As per current recommendations, spironolactone should be used with caution in patients with an eGFR <45 mL/min/1.73 m2 when plasma potassium concentration is >4.5 mmol/L.1 In patients treated with spironolactone, plasma potassium and eGFR must be closely monitored, at least annually or at 3- to 6-month intervals thereafter. However, the AMBER (Patiromer versus placebo to enable spironolactone use in patients with resistant hypertension and chronic kidney disease; ClinicalTrials.gov identifier: NCT03071263) trial demonstrated that patiromer, by mitigating hyperkalaemia risk, enabled persistent spironolactone use in patients with stage III–IV CKD and RH.51 Another important side effect of spironolactone is gynaecomastia, breast tenderness and sexual impotence in men and menstrual abnormalities in women, owing to its affinity for progesterone and androgen receptors, leading to antiandrogenic side effects. Eplerenone, a more selective MRA, serves as an alternative option when gynaecomastia or sexual side effects limit spironolactone usage. However, it is less potent than spironolactone, requires twice-daily dosing and has smaller BP-lowering effects.2 More selective, non-steroidal MRAs are now emerging as potential alternatives. Finerenone, approved for diabetic CKD, has shown favourable renal and CV outcomes with lower rates of hyperkalaemia.52 Esaxerenone, approved for hypertension in Japan, has demonstrated potent antihypertensive effects in both monotherapy and add-on settings.53 Collectively, these newer MRAs may provide safer and more effective alternatives to spironolactone for long-term BP control in high-risk populations.
-
Step 4: BBs: if spironolactone is contraindicated or not tolerated, a BB with vasodilatory properties (e.g. nebivolol, carvedilol) can be considered, especially in patients with concomitant heart failure, coronary artery disease or tachyarrhythmias.2
-
Step 5: Alpha-blockers (e.g. doxazosin) or central alpha-2 agonists (e.g. clonidine, guanfacine): these can be effective but are limited by side effects, such as orthostatic hypotension with alpha-blockers, and rebound hypertension, sedation and dry mouth with clonidine. A major drawback is rebound hypertension if withdrawn abruptly, thereby requiring careful dose titration and slow discontinuation.2
-
Step 6: Hydralazine or minoxidil: hydralazine (25 mg TDS [three times a day]) or minoxidil (2.5 mg BD or TDS) can be used as an add–on therapy. These drugs can cause profound hypotension. Their chronic use leads to compensatory tachycardia and fluid retention (‘pseudo-tolerance’), so they must be combined with a BB and a diuretic. Additional risks include a lupus-like syndrome with hydralazine and hypertrichosis with minoxidil.2
Emerging pharmacological therapies
Aldosterone synthase inhibitors
While MRAs are effective in the treatment of RH, they have multiple drawbacks, such as off-target steroidogenic side effects, hyperkalaemia and counter-regulatory aldosterone ‘escape’. As a result, targeting aldosterone production directly via aldosterone synthase inhibition (CYP11B2) offers a mechanistically attractive alternative, potentially avoiding these limitations and blocking both genomic and non-genomic actions of aldosterone. Early-generation aldosterone synthase inhibitors (ASIs), like osilodrostat (LCI699), inhibited not only aldosterone synthase (CYP11B2) but also 11β-hydroxylase (CYP11B1), leading to cortisol suppression and accumulation of mineralocorticoid precursors, thereby blunting their antihypertensive efficacy. Newer ASIs are far more selective, with two drugs (baxdrostat and lorundrostat) showing promising results in clinical trials. Baxdrostat is a highly selective ASI (>100-fold selectivity for CYP11B2 over CYP11B1) with a ~29 h half-life (allowing once-daily dosing). In the phase II BrigHTN (Phase 2 Trial of Baxdrostat for Treatment-Resistant Hypertension; ClinicalTrials.gov identifier: NCT04519658) trial (275 patients with uncontrolled RH), baxdrostat 1–2 mg/day reduced systolic BP by ~8–11 mmHg more than placebo over 12 weeks, with ~46% of patients on 2 mg achieving BP <130/80 mmHg.54 Aldosterone levels fell, and renin levels rose, confirming on-target activity. Tolerability was generally good: a few patients (in the higher dose group) developed mild, reversible hyperkalaemia, and none developed adrenal insufficiency (note: patients with eGFR 45 mL/min/1.73 m2 were excluded from this trial). A phase III trial (BaxHTN [A Randomised, Double-Blind, Placebo-Controlled, Parallel Group Study to Assess the Efficacy and Safety of Baxdrostat in Participants With Uncontrolled Hypertension on Two or More Medications Including Participants With Resistant Hypertension; ClinicalTrials.gov identifier: NCT06034743], 794 patients) recently reported that baxdrostat (1 or 2 mg) lowered SBP by ~9–10 mmHg more than placebo at 12 weeks.55 The BP effect was evident by 4 weeks and sustained through the study period. Hyperkalaemia occurred in ~2–3% of baxdrostat-treated patients versus <1% on placebo. Lorundrostat is an oral, highly selective ASI, which has shown more promising and consistent BP-lowering effects in clinical trials, especially in obesity-related hypertension and suppressed renin activity. The Target-HTN (A Randomized, Double-blind, Placebo-controlled, Dose-ranging, Multicenter Phase 2 Study to Evaluate the Safety, Efficacy, and Tolerability of MLS-101 in Subjects With Uncontrolled Hypertension; ClinicalTrials.gov identifier: NCT05001945) phase II trial and Advance-HTN (A Randomized, Double-Blind, Placebo Controlled, Parallel Arm, Multicenter, Phase 2 Study to Evaluate the Efficacy and Safety of Lorundrostat in Subjects With Uncontrolled Hypertension on a Standardized Medication Regimen; ClinicalTrials.gov identifier: NCT05769608) phase IIb trial confirmed that lorundrostat reduced 24 h average SBP in participants with RH more than placebo, particularly in patients with obesity.56,57 The recently published phase III LAUNCH-HTN (A Randomized, Double-Blind, Placebo Controlled, Parallel Arm, Multicenter Phase 3 Study to Evaluate the Efficacy and Safety of Lorundrostat in Subjects With Uncontrolled and Resistant Hypertension; ClinicalTrials.gov identifier: NCT06153693) trial further confirmed that 50 mg of lorundrostat once daily significantly reduced SBP versus placebo (16.9 versus 7.9 mmHg) at week 6 of therapy.58
Clinical implications: ASIs provide proof-of-concept that targeting aldosterone production can substantially lower BP in RH, potentially with fewer side effects than spironolactone. However, their long-term safety and impact on clinical outcomes remain to be determined.
Endothelin receptor antagonists
Endothelin (ET)-1 is a potent vasoconstrictor that contributes to hypertension, vascular injury and aldosterone release. Endothelin A (ETA) receptor activation promotes vasoconstriction, sodium retention and fibrosis, while endothelin B (ETB) receptor stimulation has protective effects (vasodilation, natriuresis and anti-inflammation). Thus, ETA blockade or balanced ETA/ETB antagonism is attractive in RH. First-generation ETA-selective antagonists (e.g. darusentan) reduced BP by ~7 mmHg but caused significant oedema/fluid retention in a large proportion of patients (28%), limiting their clinical utility.59 Other ETA blockers (e.g. avosentan, atrasentan) showed renal benefits (reduced proteinuria) but were halted in trials due to high rates of fluid overload and heart failure. These outcomes underscored that blocking ETA alone can lead to counter-regulatory fluid retention. Dual ETA/ETB antagonists were developed to mitigate this issue. Aprocitentan is a dual ETA/ETB antagonist. In preclinical studies, it lowered BP without impairing renal function (especially when combined with RAAS blockade). Early-phase clinical studies showed a long half-life (~44 h) and only mild, non-dose-dependent fluid retention.60 In a phase II trial (490 patients with essential hypertension), aprocitentan 12.5–25 mg/day reduced office SBP by 7–10 mmHg versus placebo, with less oedema than seen with earlier ETA-selective drugs.61 The phase III PRECISION (Dual endothelin antagonist aprocitentan for resistant hypertension; ClinicalTrials.gov identifier: NCT03541174) trial (730 patients with true RH on standardized triple therapy) found that aprocitentan 12.5–25 mg/day further reduced office SBP by 3.7 mmHg versus placebo, confirmed by a 5.9 mmHg greater reduction in 24 h ambulatory blood pressure (ABP).62 Notably, BP lowering was sustained through 48 weeks of therapy, and significant reductions were observed in night-time BP (an important prognostic marker), as well as in proteinuria. Fluid retention occurred in 9–18% of patients but was generally mild and manageable with diuretics.
Clinical implications: these results confirm that ET-1 plays a role in RH and associated cardiorenal disease. While first-generation ETA-selective drugs were limited by fluid overload, aprocitentan’s dual receptor blockade provides a more balanced approach, yielding sustained BP reductions and potential renal benefits with an acceptable safety profile. Nonetheless, monitoring for fluid retention is still required, particularly in patients susceptible to volume overload (those with CKD or heart failure).
Zilebesiran: a small interfering RNA approach to renin–angiotensin–aldosterone system suppression
Zilebesiran is an investigational small interfering RNA therapy designed to silence hepatic angiotensinogen synthesis, thereby reducing the substrate for the RAAS cascade. Early-phase trials (phase I and KARDIA-1 [RNA Interference With Zilebesiran for Mild to Moderate Hypertension]; ClinicalTrials.gov identifier: NCT04936035) demonstrated dose-dependent, sustained reductions in ambulatory systolic BP (≥10 mmHg) after single subcutaneous doses, with effects lasting up to 6 months.63 Its safety profile has been favourable to date, with mostly mild injection-site reactions and no serious renal or electrolyte complications reported. Zilebesiran is currently being evaluated as an add-on therapy (KARDIA-2 [Add-On Treatment With Zilebesiran for Inadequately Controlled Hypertension] trial; ClinicalTrials.gov identifier: NCT05103332) in patients with uncontrolled hypertension. Results showed that zilebesiran achieved clinically significant and sustained 24 h systolic BP reductions at 3 and 6 months compared with placebo, with a generally favourable safety profile.64 Because of its long-acting upstream RAAS inhibition, zilebesiran holds promise in RH, particularly in patients inadequately controlled by conventional agents and those with adherence challenges.
Device-based treatment of resistant hypertension
Renal denervation therapy
Over the past two decades, interventional approaches to RH have been investigated as adjuncts to lifestyle modification and pharmacological therapy. Among these, catheter-based RDN has emerged as the most extensively studied and clinically adopted. The rationale for RDN stems from recognition of the SNS’s critical role in RH pathophysiology. The renal sympathetic nerves, located in the adventitia of the renal arteries, comprise both efferent fibres, which modulate renin release, sodium retention and renal haemodynamics and afferent fibres, which provide feedback to central sympathetic centres. Hyperactivity of this axis contributes to both the initiation and maintenance of elevated BP in many patients. Ablation of these nerves using catheter-based technologies aims to disrupt this maladaptive signalling, thereby lowering BP.65
Evolution of renal denervation: from early promise to neutral trials and reappraisal
Initial open-label studies of radiofrequency (RF) RDN (Table 4), notably the SYMPLICITY HTN-1 (Renal Denervation in Patients With Uncontrolled Hypertension-1; ClinicalTrials.gov identifier: NCT00483808 and NCT00664638) and SYMPLICITY HTN-2 (Renal Denervation in Patients With Uncontrolled Hypertension-2; ClinicalTrials.gov identifier: NCT00888433) trials, demonstrated substantial reductions in office BP, generating enthusiasm for the therapy.66–80 However, the pivotal SYMPLICITY HTN-3 (Renal Denervation in Patients With Uncontrolled Hypertension-3; ClinicalTrials.gov identifier: NCT01418261) trial, the first large, randomized, sham-controlled study, failed to demonstrate superiority of RDN over sham at 6 months.66 This result led to widespread scepticism and a pause in clinical adoption. Several explanations for the neutral findings included suboptimal ablation techniques in complete circumferential nerve disruption, operator inexperience, heterogeneity in adherence to background pharmacotherapy and an overreliance on office BP rather than ambulatory BP as the primary outcome. Subsequent generations of trials were carefully redesigned to address these limitations. Key innovations included the use of multi-electrode RF catheters capable of delivering more complete circumferential ablation, ultrasound-based circumferential ablation systems, improved operator training and adoption of ABPM as a primary endpoint. Moreover, studies were stratified into patients off antihypertensive medications (to avoid confounding by adherence) and those on stable background regimens. These methodological refinements ushered in a second wave of trials, such as the SPYRAL HTN ON-MED trial (Global Clinical Study of Renal Denervation With the Simplicity Spyral Multi-Electrode Renal Denervation System in Patients With Uncontrolled Hypertension on Standard Medical Therapy; ClinicalTrials.gov identifier: NCT02439775) and RADIANCE-HTN (Endovascular Ultrasound Renal Denervation to Treat Hypertension; ClinicalTrials.gov identifier: NCT02649426) programmes, which consistently demonstrated modest but clinically meaningful BP reductions compared with sham control.81,82
Table 4: Characteristics and outcomes of renal denervation trials in resistant hypertension66–78
| Trial [NCT number] (year)/author/n | RDN system | Standard medications | Sham control | Follow-up duration (months) | Δ24 h SBP RDN (mmHg) | Δ24 h SBP control (mmHg) | p-value |
| Symplicity HTN-3 [NCT01418261]/Bhatt et al./(2014)/n=1,35366 | Symplicity Flex (single) | No (≥3 drugs) | Yes | 6 | -6.75 | -4.79 | 0.26 |
| DENER HTN [NCT01570777]/(2015)/n=10677 | Symplicity Flex (single) | Yes | No | 6 | -15.8 (daytime) | -9.9 (daytime) | 0.03 |
| DENERV HTA [NCT02039492]/(2016)/n=2478 | Symplicity Flex (single) | No | No | 6 | -5.1 | -23.6 | 0.01 |
| Prague-15 [NCT01560312]/Rosa et al. (2015)/n=10667 | Symplicity Flex catheter (Medtronic) (single) | No | No | 6 | -8.6 | -8.1 | 0.87 |
| Symplicity FLEX [NCT01656096]/ Desch et al. (2015)/n=7168 | Symplicity Flex (single) | No | Yes | 6 | -7.0 | -3.5 | 0.15 |
| ReSET [NCT03307343]/ Mathiassen et al. (2016)/n=6969 | Symplicity Flex (single) | No | Yes | 3 | -6.2 (daytime) | -6.0 (daytime) | 0.95 |
| WAVE IV [NCT02029885]/ Schmieder et al. (2018)/n=8170 | External ultrasound | No | Yes | 6 | -18.9 (office) | -13.2 (office) | 0.18 |
| RADIANCE-HTN TRIO [NCT02649426]/(2021)/Azizi et al./n=98971 | Paradise RDN system (ReCor Medical) | Yes | Yes | 2 | -8.0 (daytime) | -3.0 (daytime) | 0.02 |
| RADIOSOUND-HTN [NCT02920034]/(2019)/Fengler et al./n=12072 | Paradise versus Spyral main versus Spyral main + branch | No | No (three active arms) | 3 | -13.2 (Paradise) | -6.7 (Spyral main); -8.3 (Spyral main + branch) | 0.04 |
| REQUIRE [NCT02918305]/(2022)/Kario et al./n=7273 | Paradise | No | Yes (single-blind) | 3 | -6.6 | -6.5 | 0.97 |
| TARGET BP I [NCT02910414]/(2024)/Kandzari et al./n=14574 | Peregrine (Alcohol RDN) | Yes | Yes | 6 | -10.0 (Ambulatory) | -6.8 (Ambulatory) | 0.04 |
| SMART [NCT02761811]/(2024)/Wang et al./n=11075 | RF catheter (SyMap Medical [Suzhou], LTD, Suzhou, China) | Yes | Yes (single-blind) | 6 | -10.8 | -10.0 | >0.05 |
| Iberis-HTN Trial [NCT02901704]/(2024)/Jiang et al./n=10776 | Multielectrode, unipolar Iberis RDN catheter and generator system (AngioCare, Shanghai, China) | Yes | Yes | 6 | -13.0 | -3.0 | <0.001 |
RDN = renal denervation; RF = radiofrequency; SBP = systolic blood pressure.
Mechanisms and techniques of renal denervation
Two principal technologies have been validated for RDN.65
-
Radiofrequency RDN (rRDN) involves percutaneous catheter access and delivery of multiple low-power RF ablations in a spiral fashion within the main and branch renal arteries. The most widely studied platform is the Symplicity Spyral™ Renal Denervation System (Medtronic Inc., Santa Rosa, CA, USA), which employs four radiopaque electrodes arranged in a helical configuration at the catheter tip to emit RF energy and achieve multi-site ablation.
-
Ultrasound RDN (uRDN) delivers circumferential thermal energy via a balloon catheter with saline cooling, designed to achieve consistent circumferential ablation of sympathetic nerves in the main renal arteries. uRDN is performed with the Paradise Renal Denervation System (ReCor Medical Inc., Palo Alto, CA, USA), which incorporates a balloon at the distal tip surrounding an ultrasound-emitting core. This design enables consistent circumferential ablation of sympathetic nerves within the main renal arteries. Notably, clinical evidence suggests that uRDN performed in the main renal arteries achieves BP reductions comparable to rRDN when ablations are extended to both the main and distal branches. Both procedures are performed under angiographic guidance, typically via femoral arterial access, and last approximately 1 h. Importantly, procedural complications are rare, with serious vascular or renal events occurring in <1% of cases in contemporary RCTs.
Evidence from randomized controlled trials
The efficacy of RDN in patients with RH despite treatment with at least three drugs at >50% of the maximal recommended dose has been evaluated in 13 RCTs, which have now been summarized in Table 4.66–78 Among the earliest studies, three trials using the Symplicity Flex System reported no significant difference in 24 h BP between RDN and sham groups.66–68 This lack of efficacy was due to the inherent limitations of the unipolar catheter, resulting in incomplete denervation. Additionally, greater-than-expected reductions in systolic BP were observed in the sham arms, likely reflecting either intensification of background pharmacotherapy outside of protocol or improved medication adherence following trial enrolment. When background therapy was standardized using fixed-dose triple combination pills and adherence was objectively monitored with biochemical drug testing, RDN showed significant benefits. In the DENER-HTN (Renal Denervation in Patients With Resistant Hypertension; ClinicalTrials.gov identifier: NCT01570777) trial, use of the Symplicity Flex System reduced daytime systolic BP by 5.9 mmHg (95% Confidence interval (CI): -11.3 to -0.5 mmHg; p=0.03) when compared with sham therapy.77 Similarly, in the RADIANCE-HTN TRIO (Ultrasound renal denervation for hypertension resistant to a triple medication pill; ClinicalTrials.gov identifier: NCT02649426) trial, the Paradise ultrasound system produced a between-group reduction in systolic BP of -4.5 mmHg (95% CI: -8.5 to -0.3 mmHg), favouring RDN.78 The RADIOSOUND-HTN (A Randomized Comparison of Ultrasound Based Versus Radiofrequency Based Catheter Ablation Techniques in Patients With Therapy Resistant Arterial Hypertension With Large Renal Arteries; ClinicalTrials.gov identifier: NCT02920034) trial, the only head-to-head randomized comparison of RF-based and ultrasound-based denervation, demonstrated a greater BP reduction with uRDN compared with rRDN.72 It should also be noted that most RCTs were limited to short-term follow-up (2–6 months). In contrast, the Global SYMPLICITY Registry has provided longer term insights, reporting sustained reductions in office systolic BP of 16.5 ± 28.6 mmHg and decreases in 24 h ambulatory systolic BP of 8.0 ± 20.0 mmHg over a follow-up period of up to 3 years.83 However, these findings must be interpreted cautiously in the absence of a sham control group.
Durability and safety
Long-term follow-up data from the SPYRAL and RADIANCE programmes, as well as large registries, confirm that BP reductions achieved with RDN are durable for at least 2–3 years.84 Sustained effects are clinically meaningful, as BP ‘regression to the mean’ often dilutes apparent benefits of antihypertensive drugs in real-world settings. Importantly, RDN does not appear to adversely affect renal function, with no excess risk of RAS or deterioration in eGFR compared with sham or medical therapy.
Clinical application
Contemporary guidelines emphasize that RDN is not a replacement for pharmacological therapy but may be considered as an adjunct in selected patients. In November 2023, the US Food and Drug Administration (FDA) approved both rRDN and uRDN devices, marking a turning point for clinical implementation.85 The AHA/ACC 2025 statement on high BP recommends considering RDN as an adjunct treatment to medications and lifestyle modification to reduce BP in selected patients with preserved kidney function (eGFR:
>40 mL/min/1.73 m²) who have RH despite optimal treatment or have intolerable side effects from additional antihypertensive drug therapy (Class IIb, LOE: B).1
The indications and contraindications of RDN have been listed in Table 5.1
Table 5: Patient selection and contraindications for renal denervation*1
| Category | Criteria |
| Indications |
|
| Contraindications |
|
*2025 ACC/AHA high blood pressure guideline.1
ACC = American College of Cardiology; ACEi = angiotensin-converting enzyme inhibitor; AHA = American Heart Association; ARB = angiotensin receptor blocker; CCB = calcium channel blocker; DBP = diastolic blood pressure; MRA = mineralocorticoid receptor antagonist; RAS = renal artery stenosis; SBP = systolic blood pressure.
Baroreceptor activation therapy
Baroreceptor activation therapy (BAT) works by electrically stimulating the baroreceptors in the carotid sinus through an implant. These receptors sense arterial pressure and relay signals to the brainstem, which, in turn, reduces SNS activity and increases parasympathetic tone. The net effect is vasodilation, reduced heart rate and lower BP.86 Early trials demonstrated significant SBP reductions (~20–30 mmHg) in RH.87 Further evidence in the form of a randomized, sham-controlled, double-blind trial (Nordic BAT study), using a second-generation BAT device (Barostim Neo; CVRx, Minneapolis, MN, USA; The Effect of BATon BP and Sympathetic Function in Resistant Hypertension [The Nordic BAT Study]; ClinicalTrials.gov identifier: NCT02572024), reported that BAT lowers BP in individuals with RH. The limitations of this therapy include:
-
invasive surgical procedure
-
device-related complications: infection, nerve injury and carotid artery issues
-
cost and the need for specialized centres, which limit availability.88
Clinical impact of resistant hypertension and healthcare costs
The economic and societal implications of RH are substantial. Compared with patients with controlled hypertension, patients with RH incur significantly higher healthcare costs, driven by increased medication burden, hospitalizations and procedural interventions.89 Quality of life is also diminished, with higher rates of depressive symptoms and treatment fatigue. Given the ageing population, rising prevalence of obesity and diabetes, and improved survival after CV events, the absolute number of individuals with RH is projected to increase, underscoring the need for effective management strategies.
Future directions and conclusions
RH remains one of the most challenging and high-risk phenotypes of hypertension, but recent advances are reshaping its management. Future strategies are increasingly focused on personalized medicine, where biomarkers such as plasma renin activity, sodium/volume status and comorbidity profiling may allow the selection of drug regimens tailored to individual pathophysiology. Novel pharmacological agents are also emerging. ASIs, including baxdrostat and lorundrostat, have shown promising BP-lowering effects, while the dual ET receptor antagonist aprocitentan has demonstrated durable efficacy in patients with uncontrolled hypertension. Other investigational therapies targeting vasopressin and sympathetic pathways are under evaluation. Device-based approaches are evolving as well: rRDN and uRDN have recently received regulatory approval, though long-term durability, cost-effectiveness and patient selection criteria remain areas of active study. In parallel, alternative neuromodulation strategies such as BAT are being refined. Importantly, improving adherence remains central to success in RH, with solutions ranging from digital health platforms and smart pill technology to simplified SPCs. Collectively, these advances promise to make future management of RH more effective, patient-centred and sustainable. On-going translational research and well-designed outcome trials will be essential to realize these opportunities and deliver measurable benefits for patients worldwide.